
Step by step
Figure 1.
Clinical view of the hopeless 21, which is only attached to the adjacent teeth by composite. Observe the severe melanosis that the patient showed although she was a caucasian spaniard.

Figure 2.
After extraction and debridement of all soft tissue remaining a full thickness “envelope” was created.
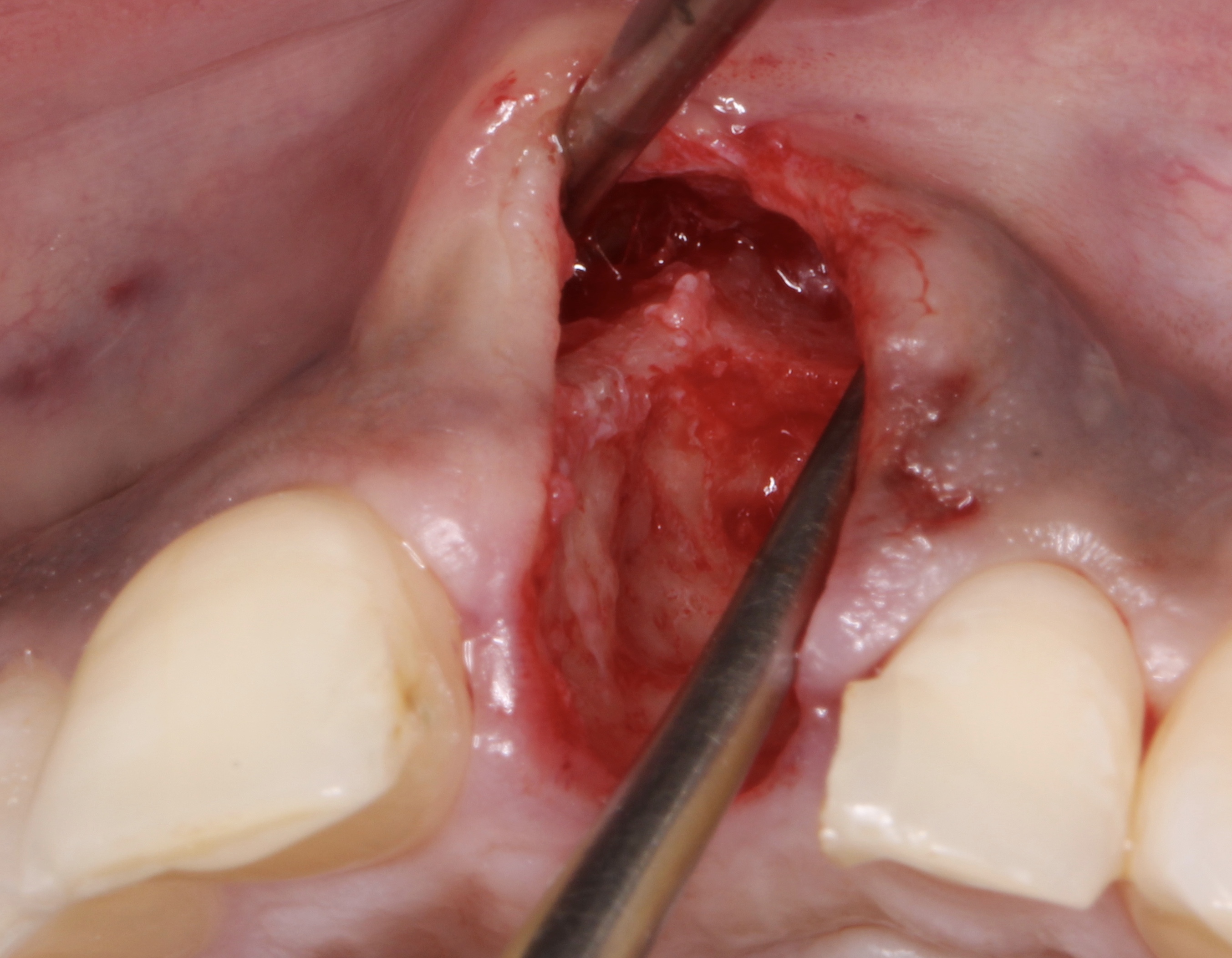
Figure 3.
After extraction and debridement of all soft tissue remaining a full thickness “envelope” was created.
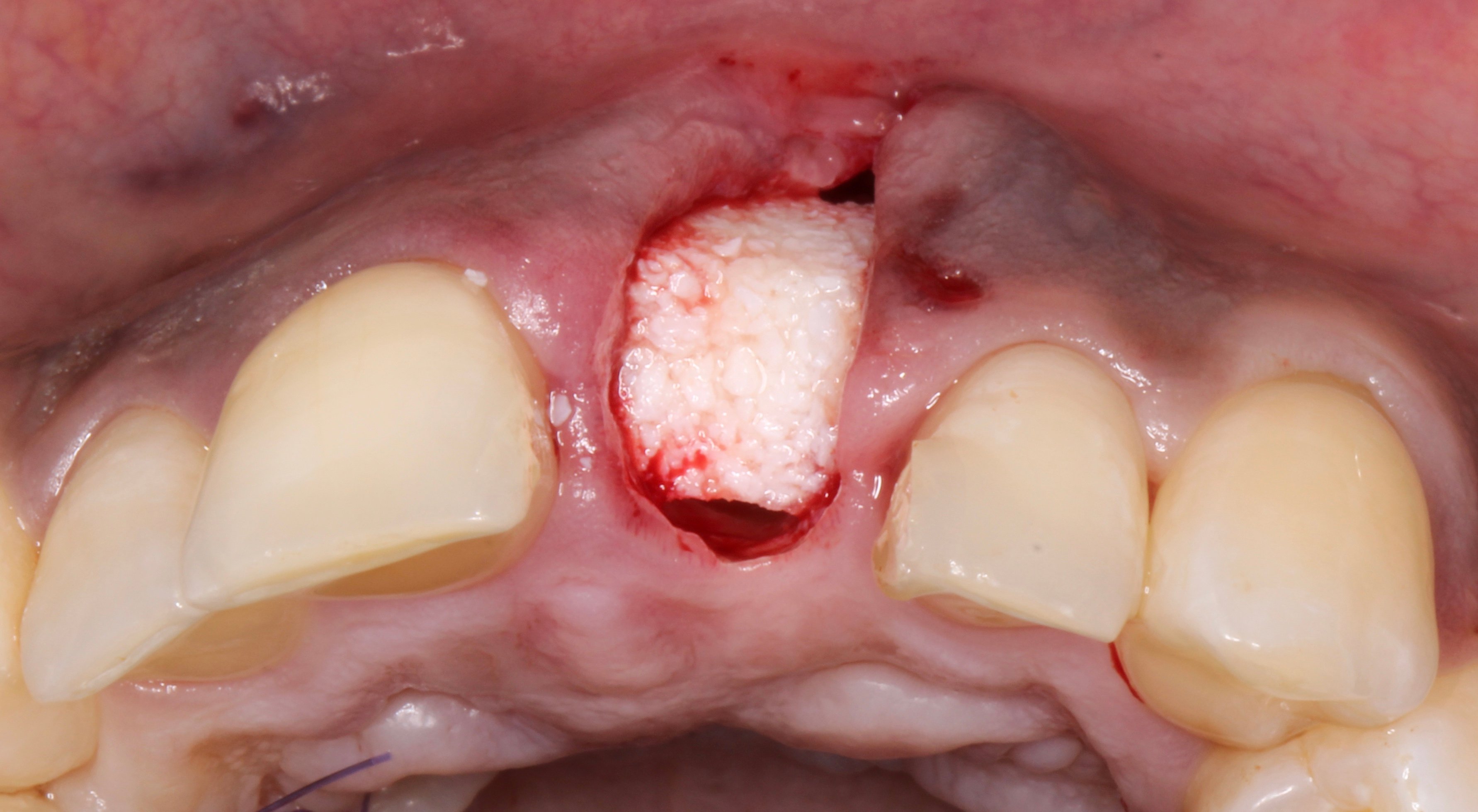
Figure 4.
Socket preservation using Xenograft (anorganic bovine hydroxylapatite-collagen) was placed and strongly condense inside the defect.
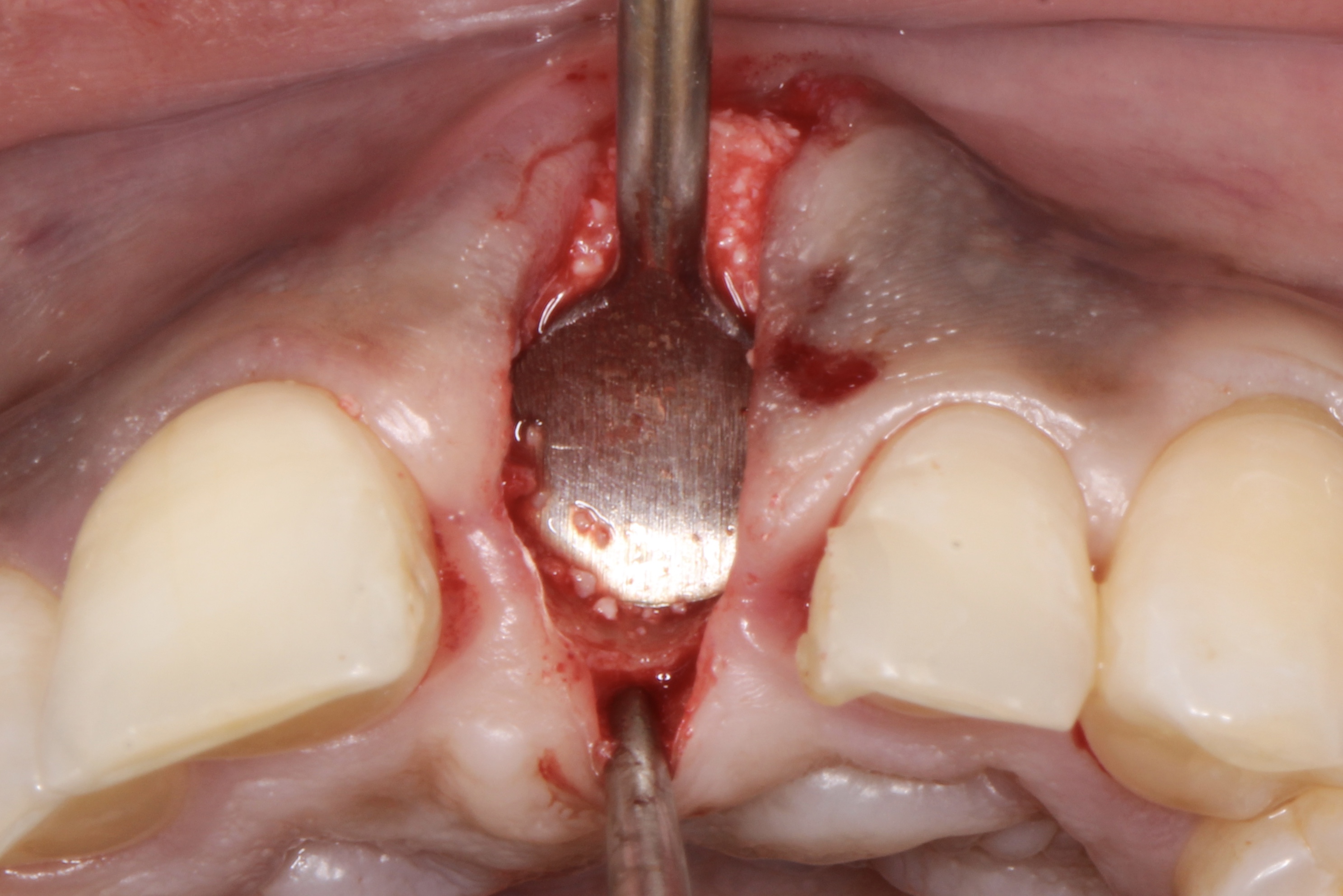
Figure 5.
Socket preservation using Xenograft (anorganic bovine hydroxylapatite-collagen) was placed and strongly condense inside the defect.

Figure 6.
A non cross-link collagen membrane was placed inside the contours of the defect covering the whole bone xenograft and stretching through the envelope.
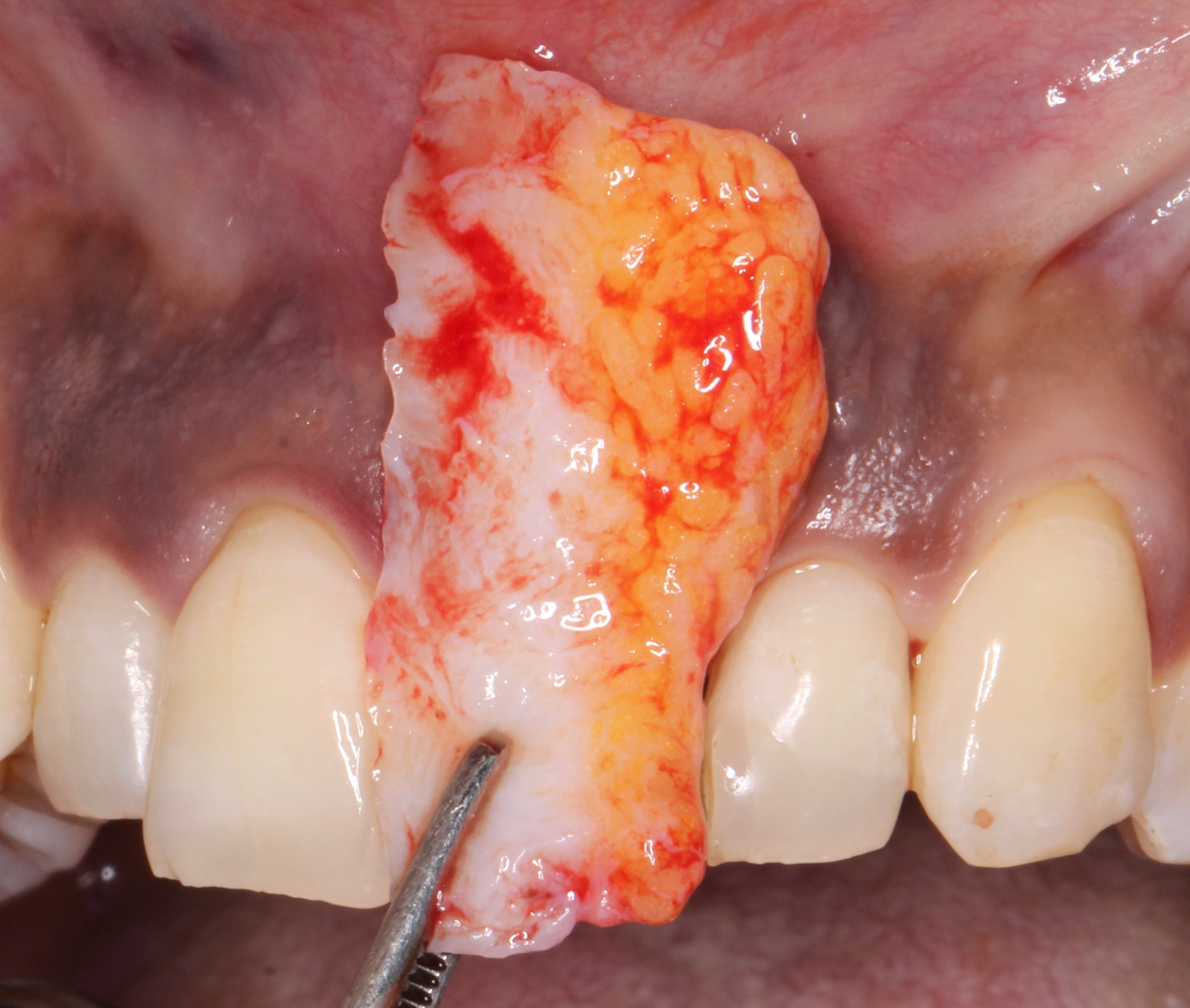
Figure 7.
A connective tissue graft was harvested from the palate and placed inside the defect ad modum “saddle” from the buccal aspect through the exposed coronal part to the palatal aspect.
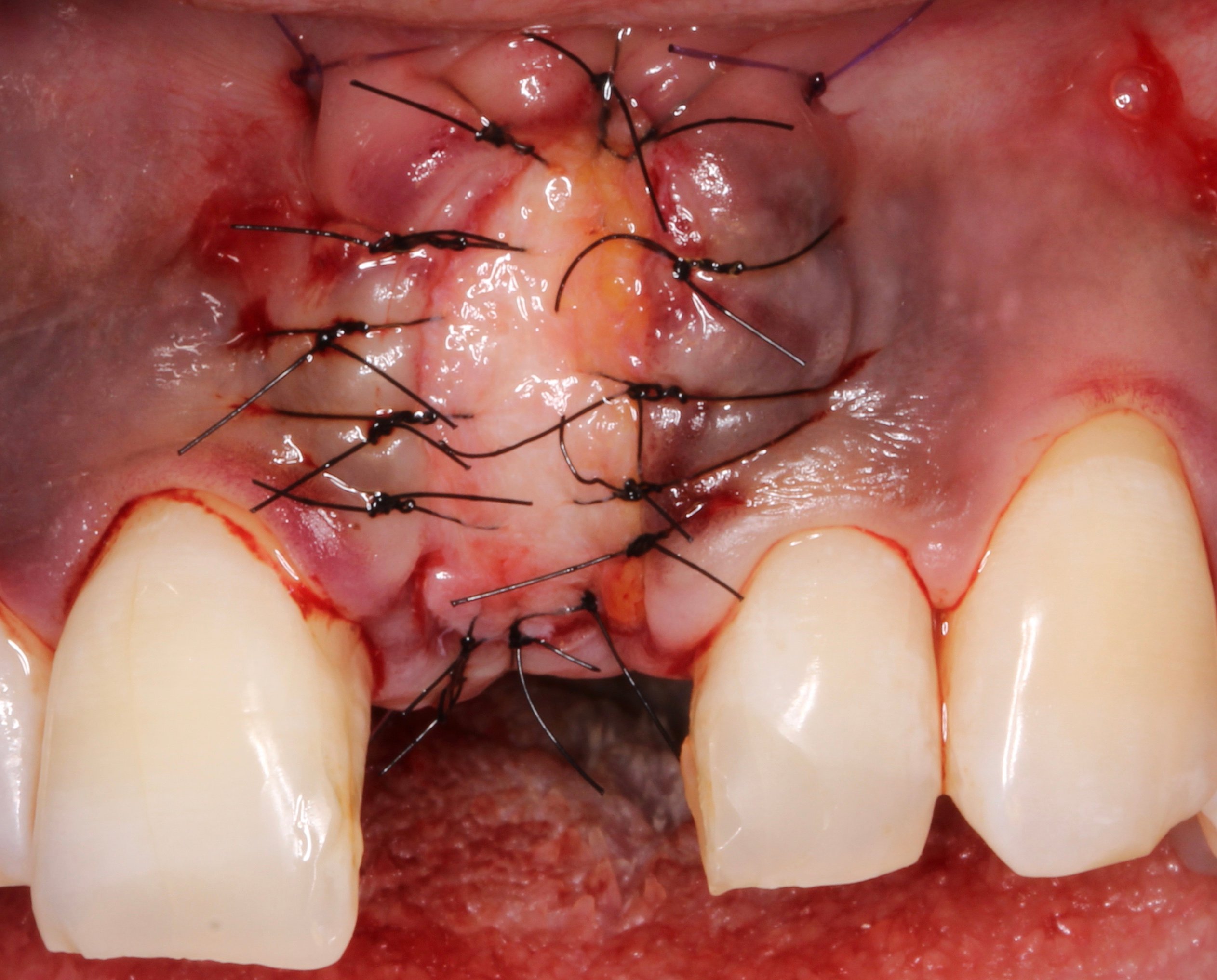
Figure 8.
A connective tissue graft was harvested from the palate and placed inside the defect ad modum “saddle” from the buccal aspect through the exposed coronal part to the palatal aspect.

Figure 9.
1 week later it was evident healing was uneventful.
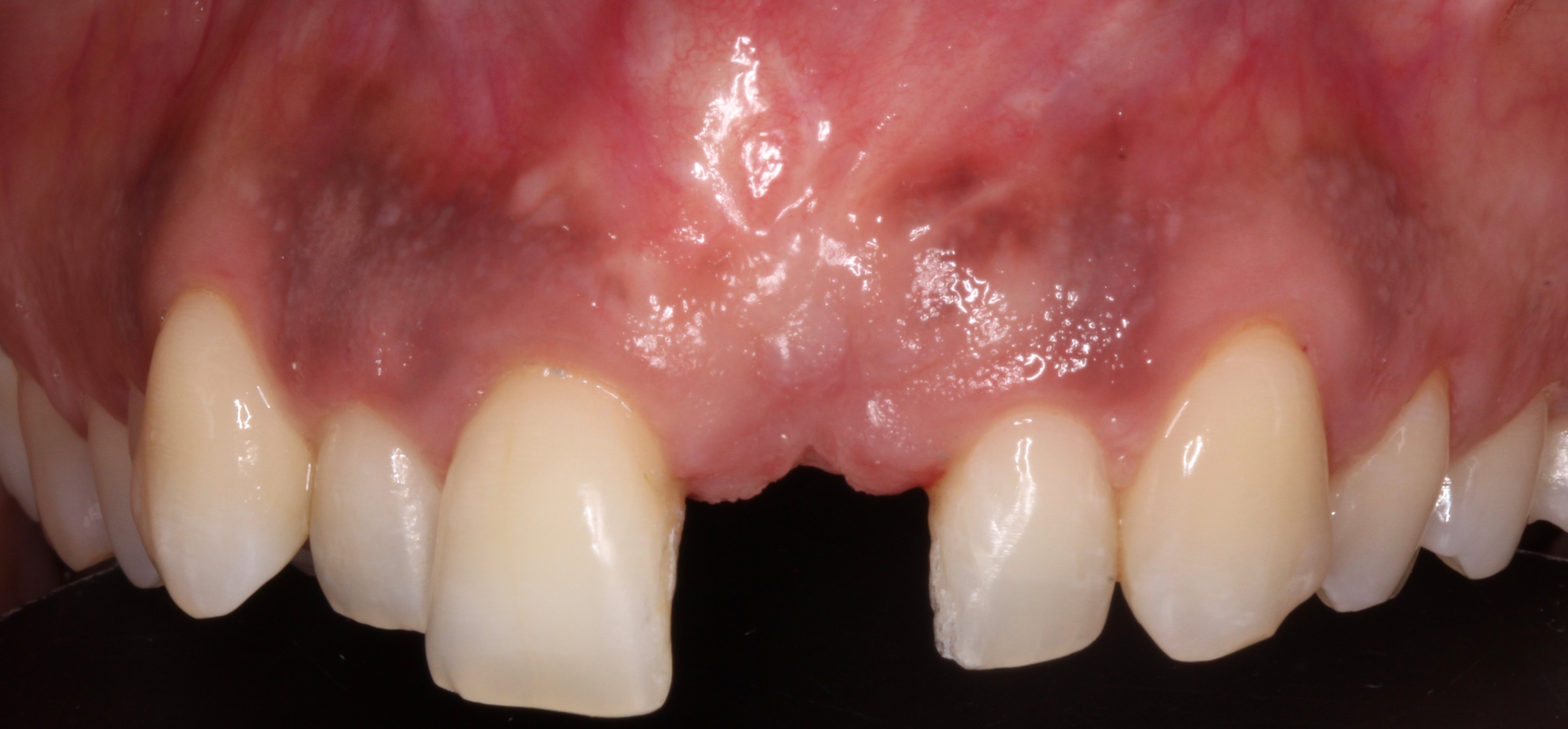
Figure 10.
9 months later: after taking a CBCT was evident that no bone gain was achieved but soft tissue status was improved due to the CTG. It was also evident that due to the lack of melanosis at the palate, the CTG which generated a new keratinised epithelium showed no melanosis at the grafted area.

Figure 11.
After raising a full thickness flap an atrophic ridge was disclosed.

Figure 12.
A Neoss ProActive® Implant 4.5 mm x 13 mm was placed.
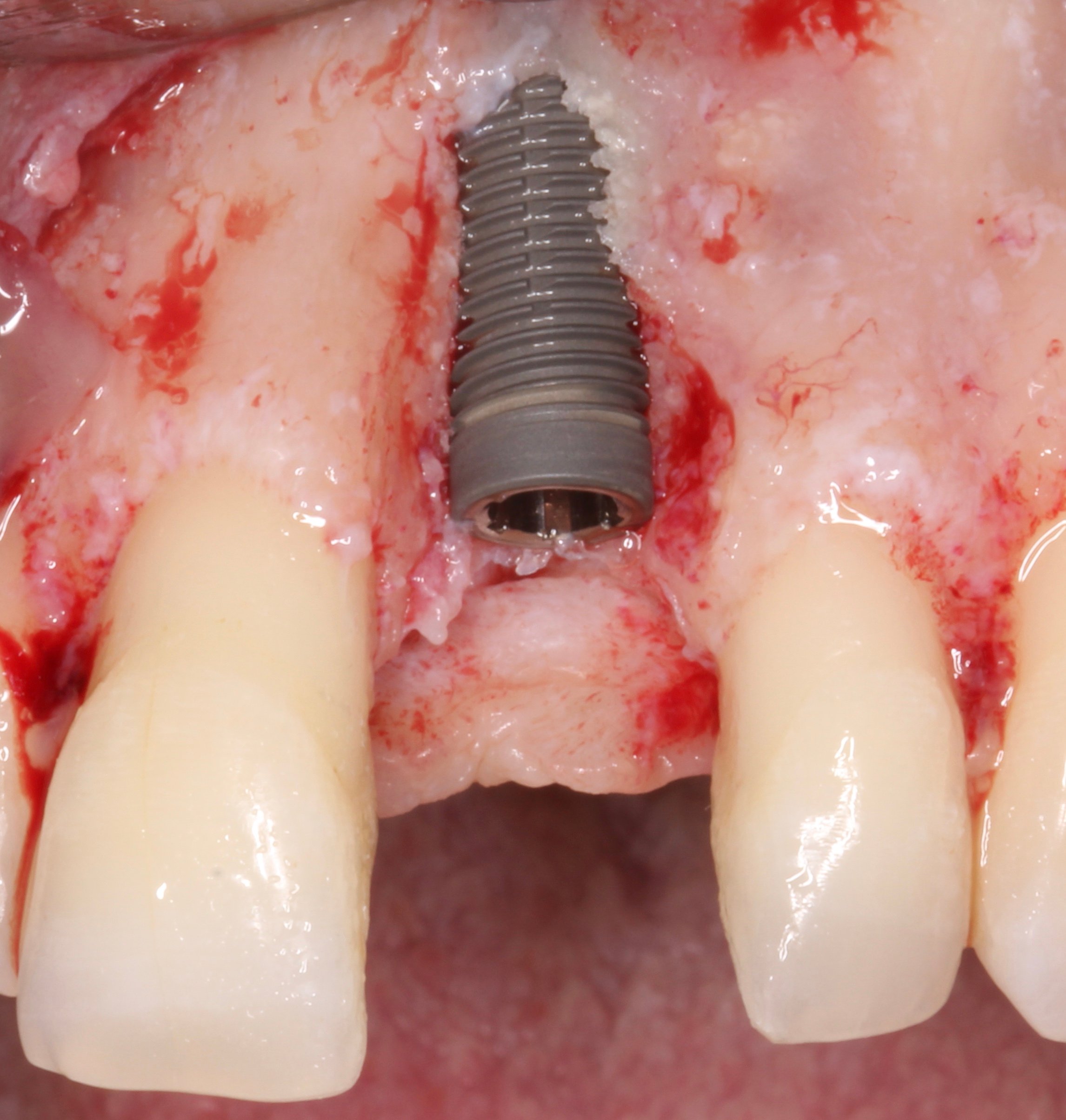
Figure 13.
Optimal 3D position of the implant resulted in a severe dehiscence. The treatment of such dehiscences is not predictable using resorbable collagen membranes so in such cases is mandatory the use of non-resorbable PTFE membranes.
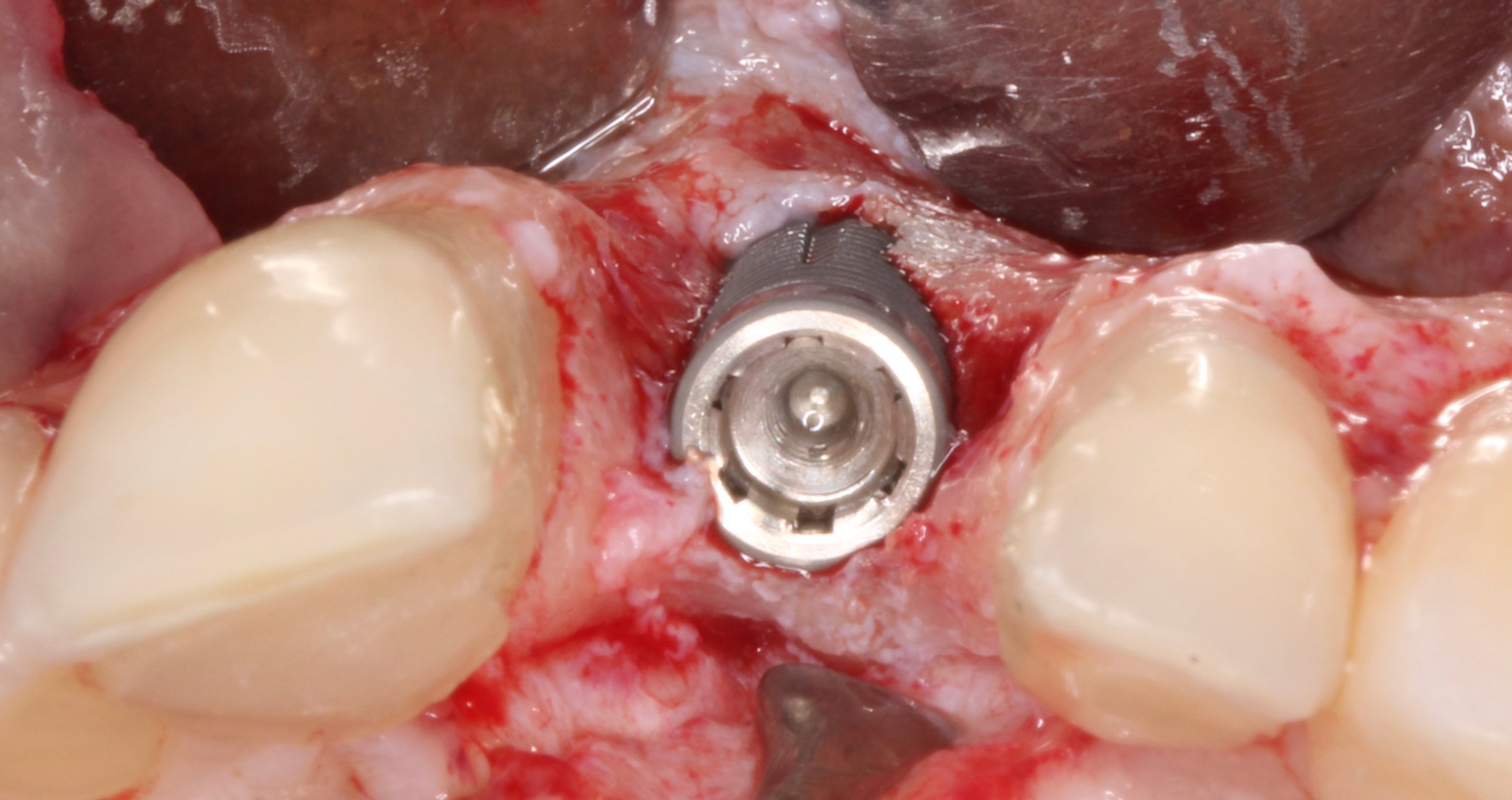
Figure 14.
Optimal 3D position of the implant resulted in a severe dehiscence. The treatment of such dehiscences is not predictable using resorbable collagen membranes so in such cases is mandatory the use of non-resorbable PTFE membranes.
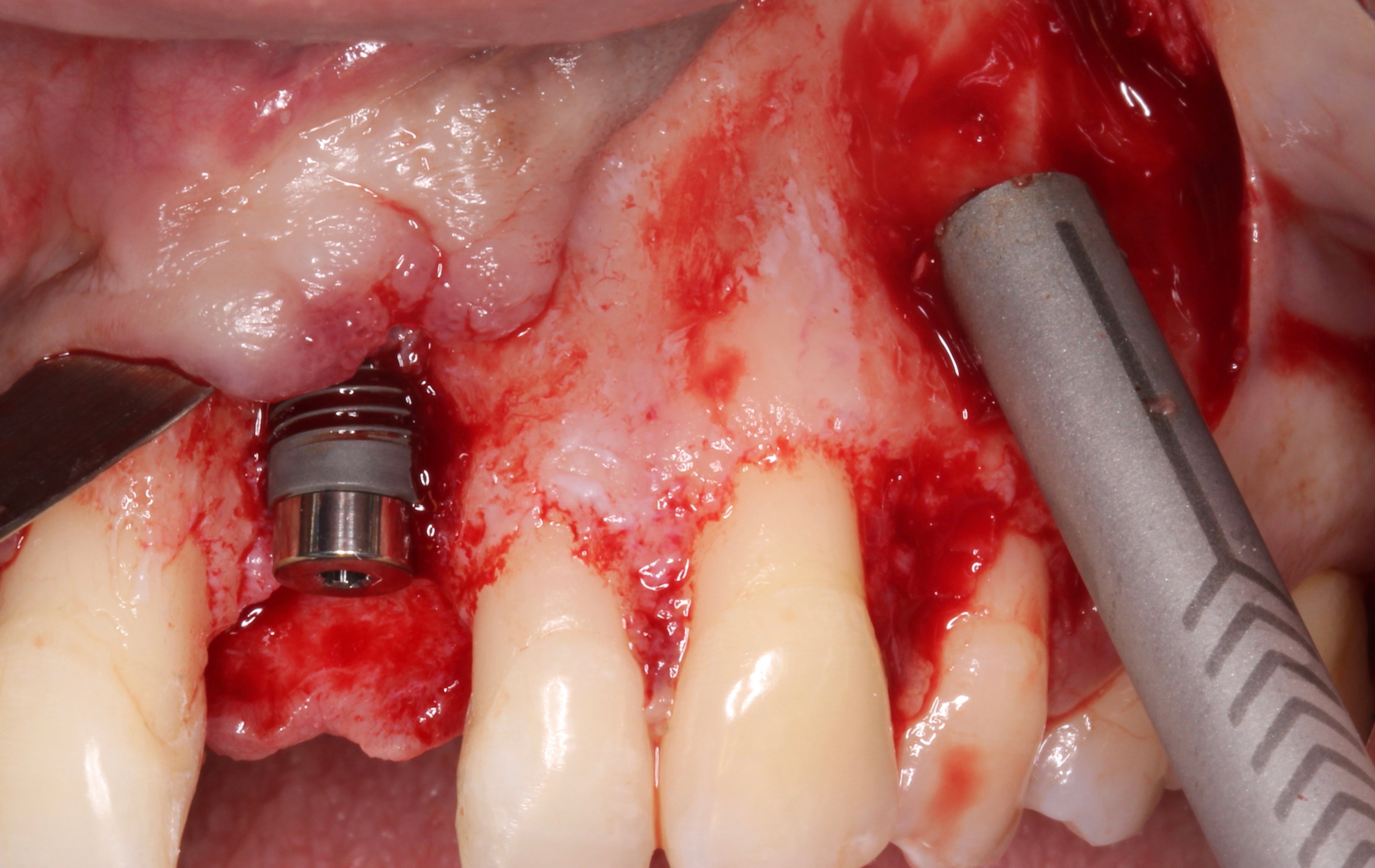
Figure 15.
Autogenous bone graft was harvested from the adjacent area using a bone scraper.
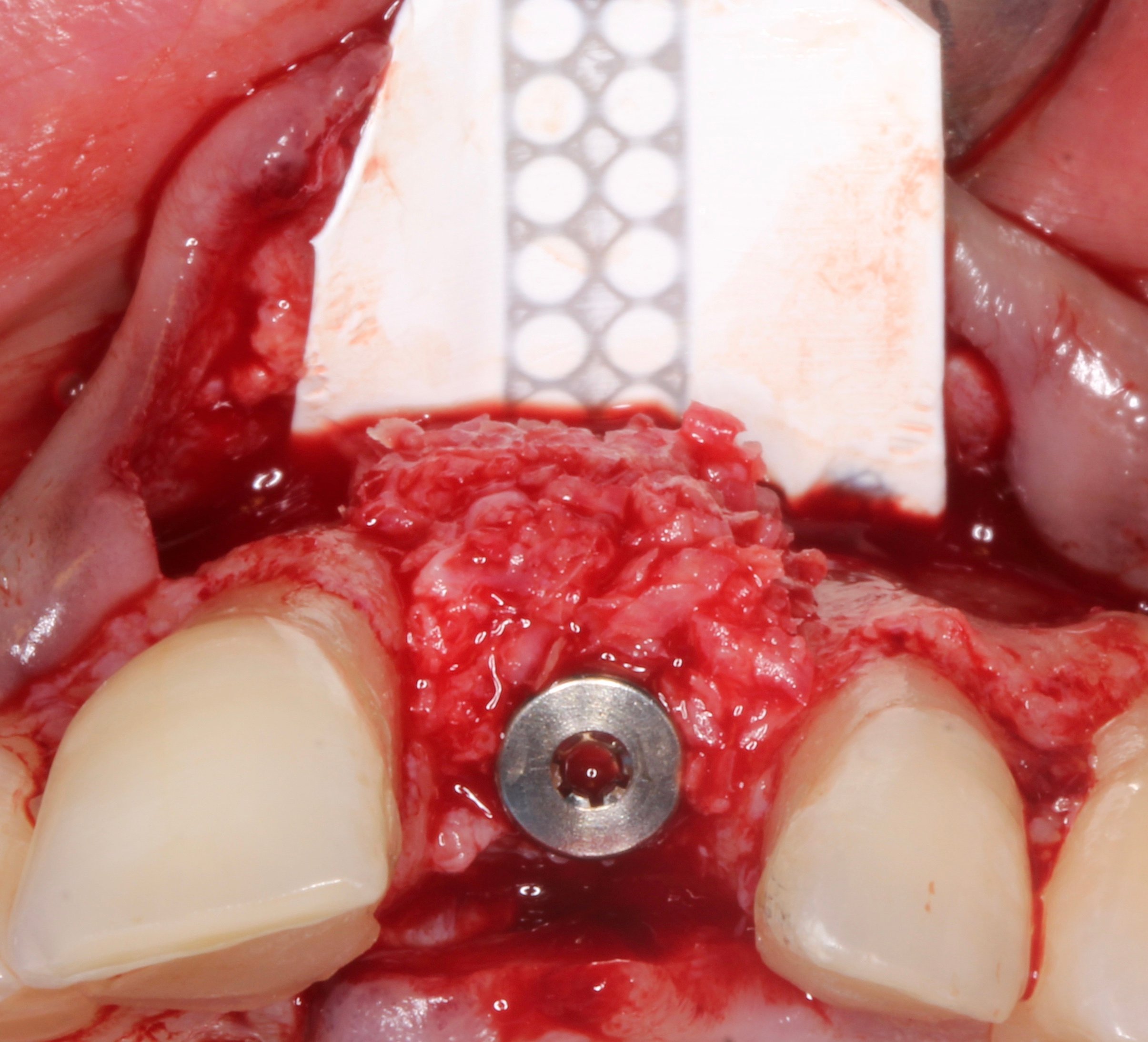
Figure 16.
After placing a 2 mm healing abutment, 100% autogenous bone was condensed to cover completely the implant surface.
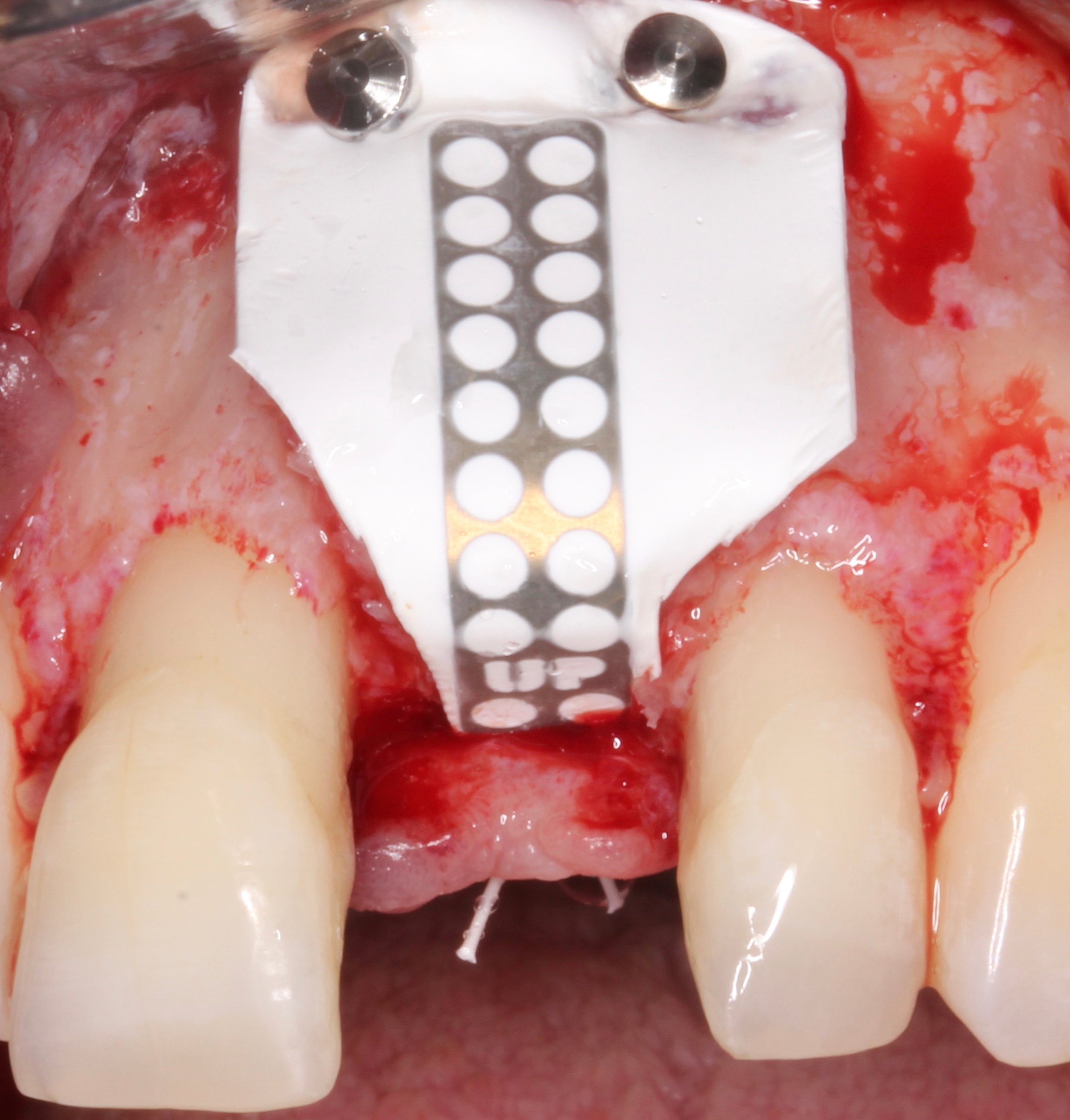
Figure 17.
A non-resorbable, Ti-reinforced NeoGen® membrane was placed covering the whole graft and fixed by tacks at buccal aspect and by a mattress suture at the palatal flap.
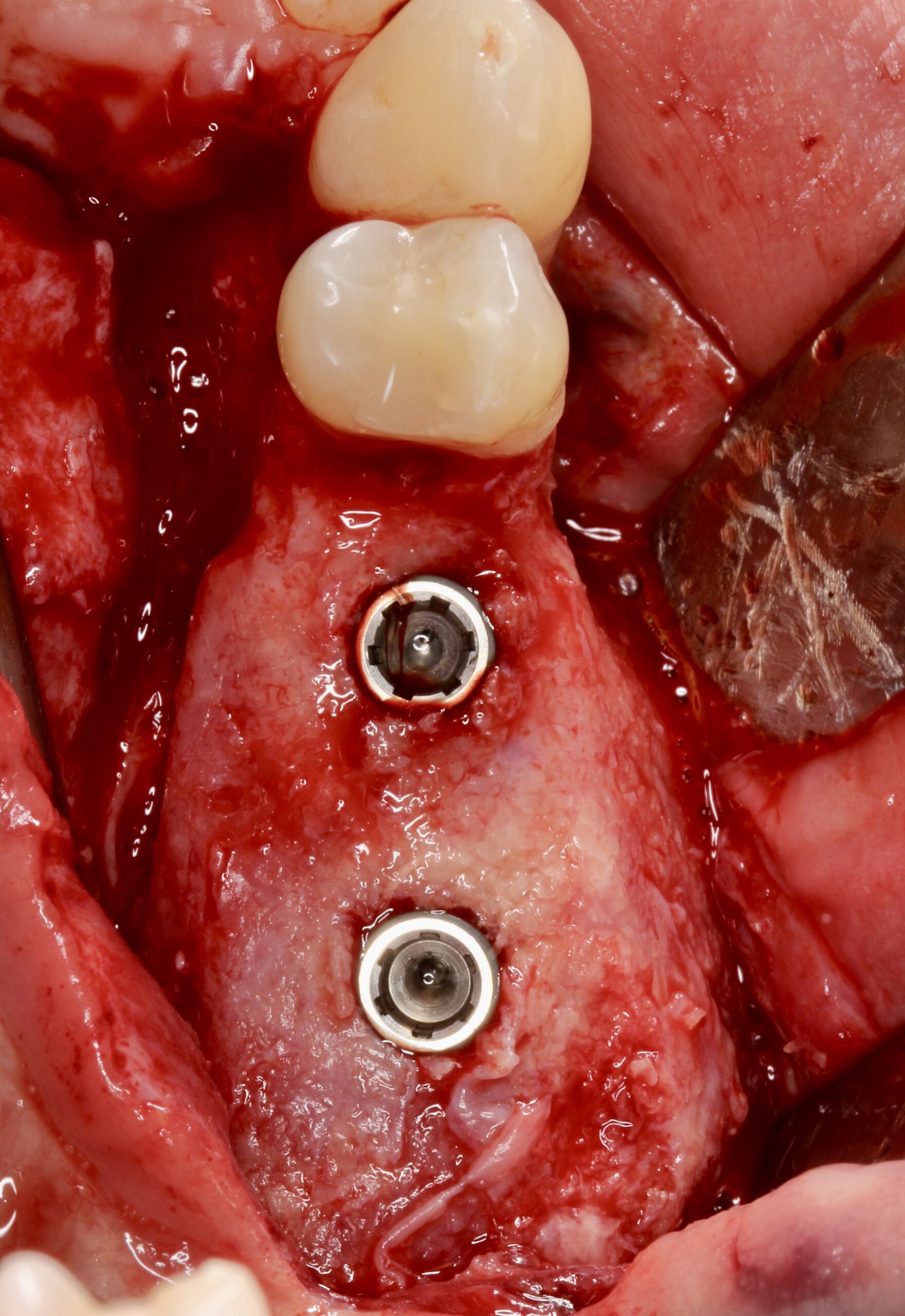
Figure 18.
Non-tension, primary closure was achieved.

Figure 19.
9 months later. Reentry was done. Notice the color of the anterior gingival. Melanosis was less evident.
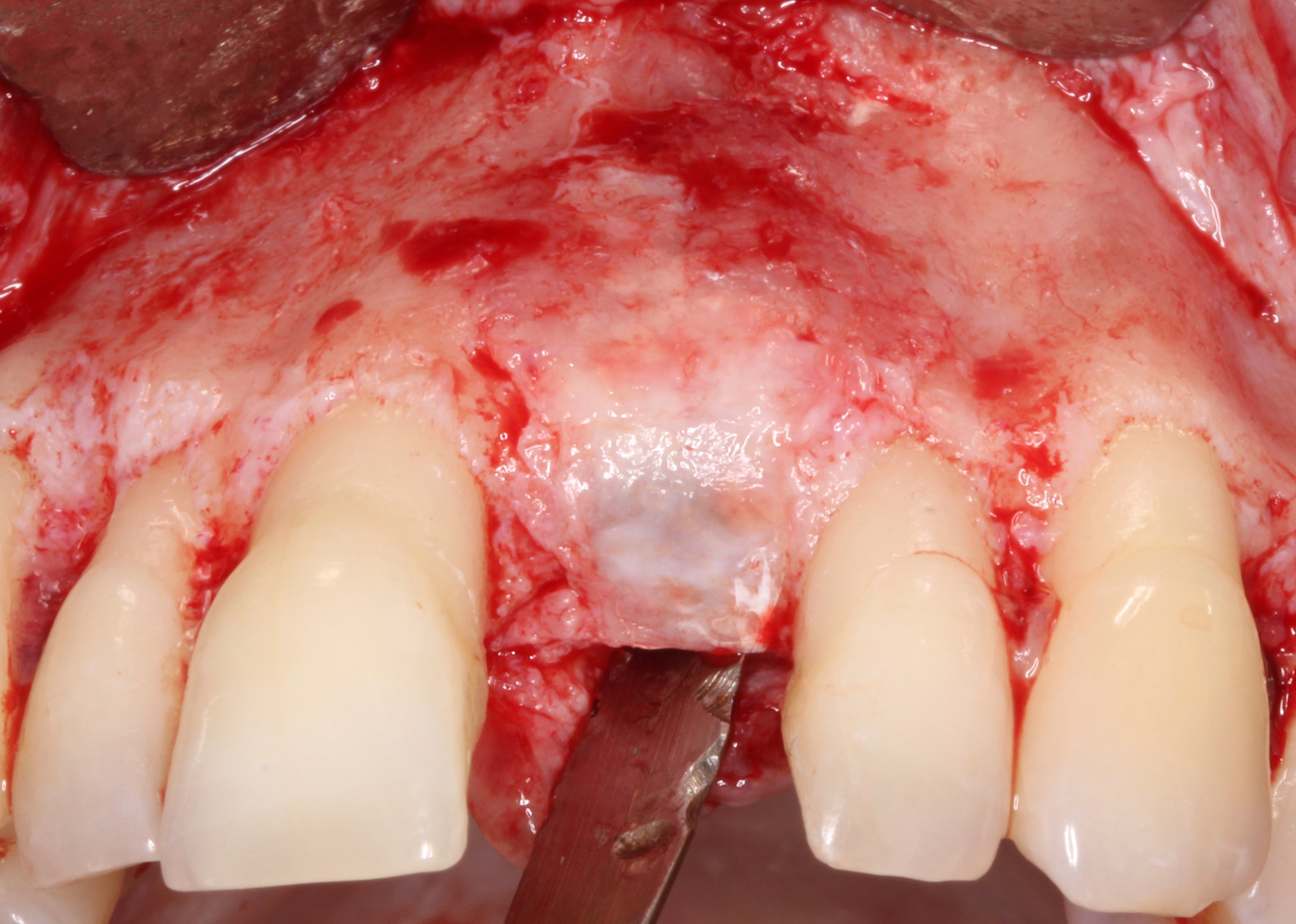
Figure 20.
After removing the membrane, complete bone regeneration was observed even covering the 2 mm healing abutment showing bone 2 mm vertical overgrowth.
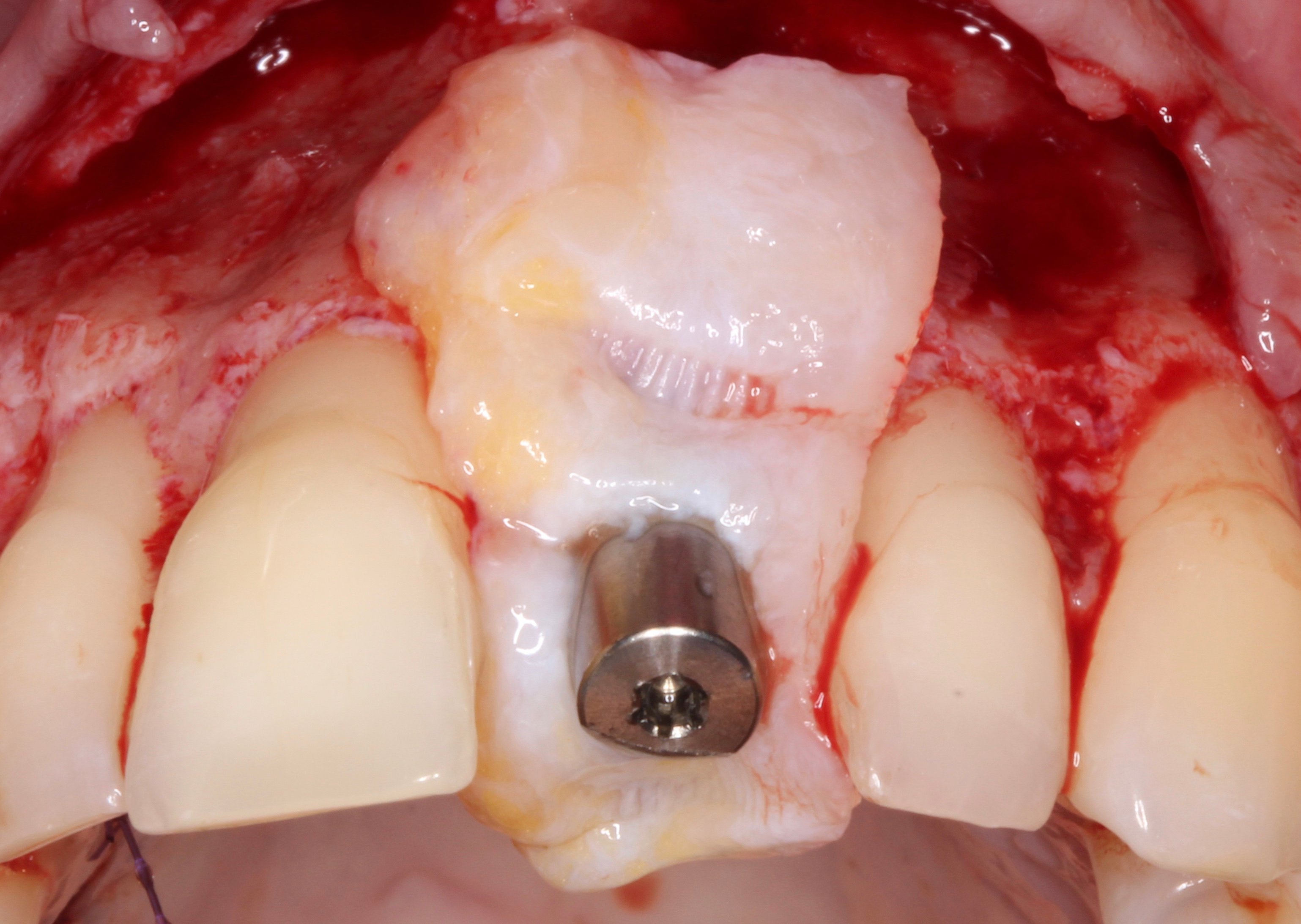
Figure 21.
A connective tissue graft was placed ad modum “poncho” around a 8 mm healing abutment.

Figure 22.
Interrupted sutures.

Figure 23.
Clinical status of the implant-supported restoration 5 years after crown delivery. Notice the complete resolution of the melanosis without signs of recidive after a peeling that was made right after crown placement.
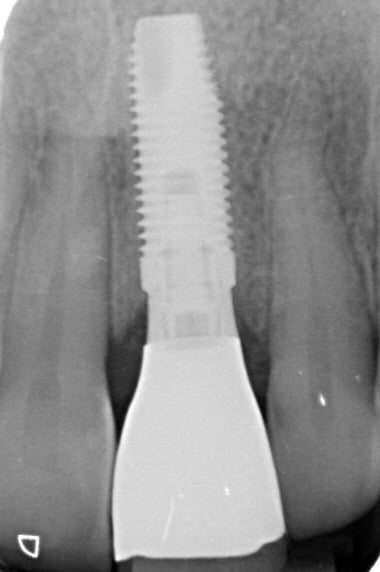
Figure 24.
X-ray image.
"Neoss ProActive® implant and NeoGen® non-resorbable, Ti-reinforced membrane is an excellent choice for the treatment of atrophic alveolar bone ridge on the aesthetic zone. The solution of bone dehiscences after implant placement by simultaneous GBR by using this protocol is fully predictable.
Dr. David González Spain 
Downloads
