
Step by step

Figure 1.
Clinical view of the right posterior maxilla showing severe bone atrophy.
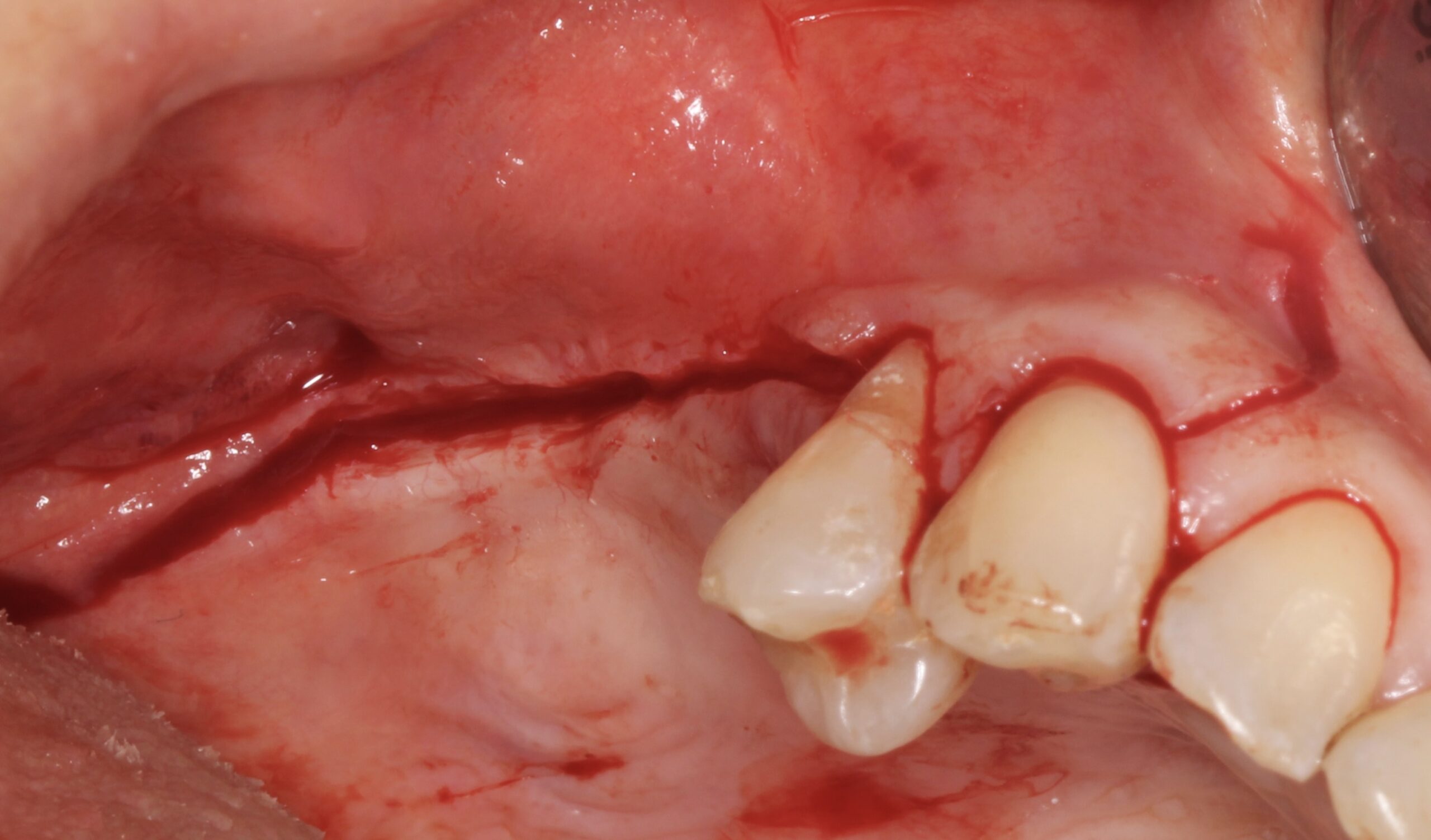
Figure 2.
Full thickness incision to expose the alveolar ridge.

Figure 3.
Severe vertical bone loss.

Figure 4.
Bone cortical cylinders were harvested from both external oblique lines and bone was also obtained by using bone scraper from both sides. The bone cylinders were crushed and mixed with the scraped bone.
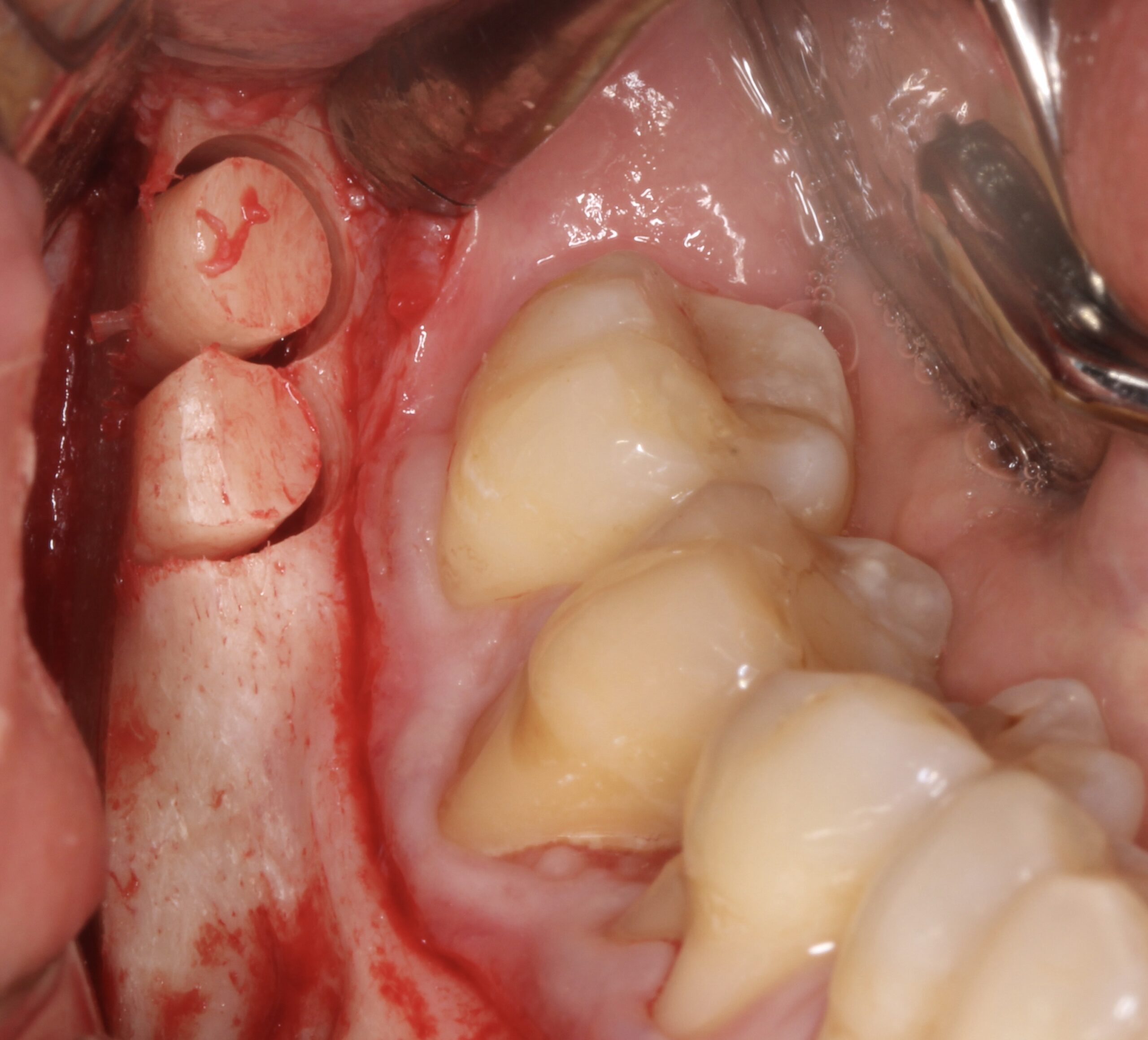
Figure 5.
Bone cortical cylinders were harvested from both external oblique lines and bone was also obtained by using bone scraper from both sides. The bone cylinders were crushed and mixed with the scraped bone.

Figure 6.
Bone cortical cylinders were harvested from both external oblique lines and bone was also obtained by using bone scraper from both sides. The bone cylinders were crushed and mixed with the scraped bone.
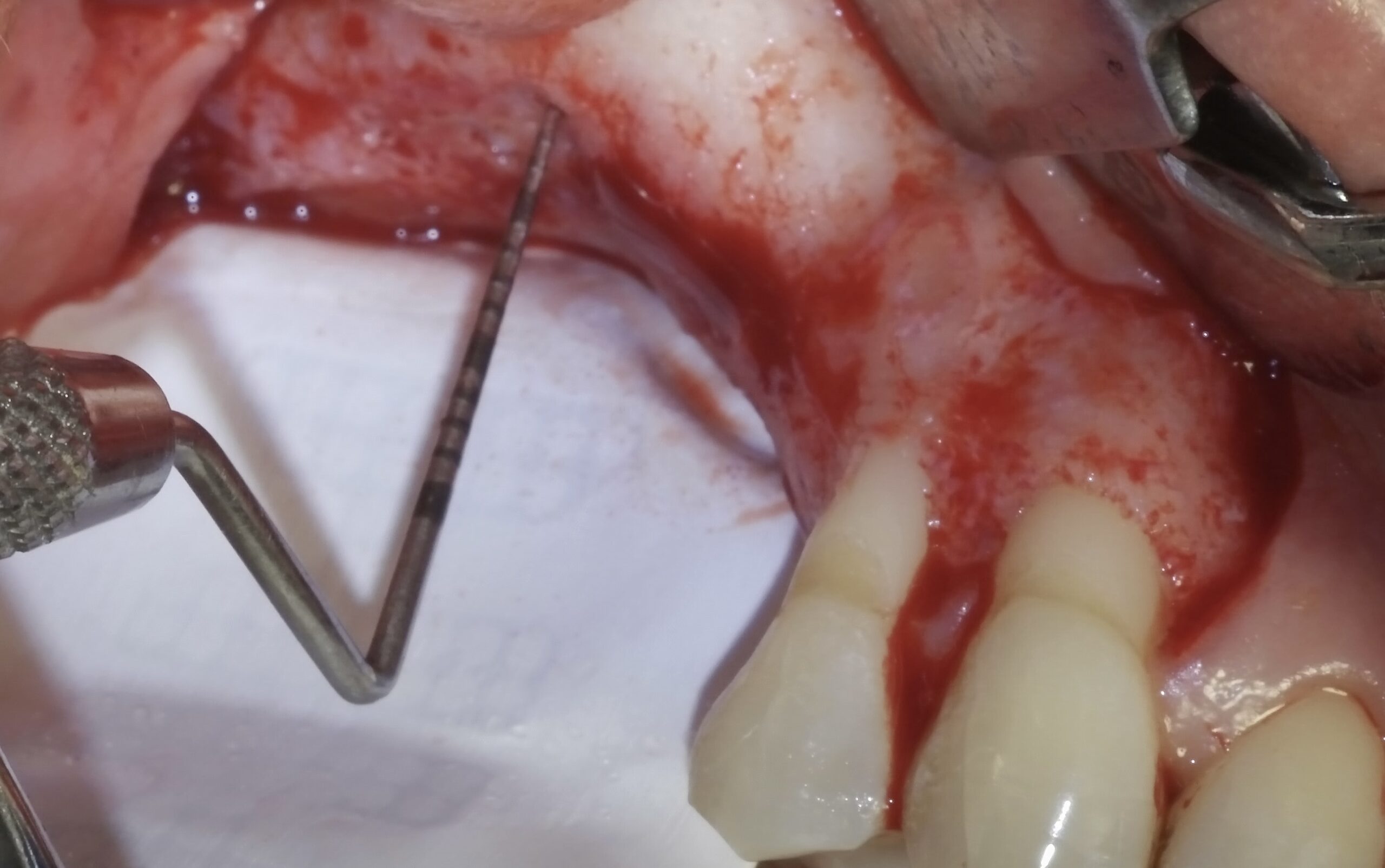
Figure 7.
A dual-PTFE, Ti-reinforced, NeoGen® membrane was fixed at palatal aspect by 3 Neoss® screws.

Figure 8.
All the harvested bone (scraped and particulated) was mixed and packed on the alveolar ridge.
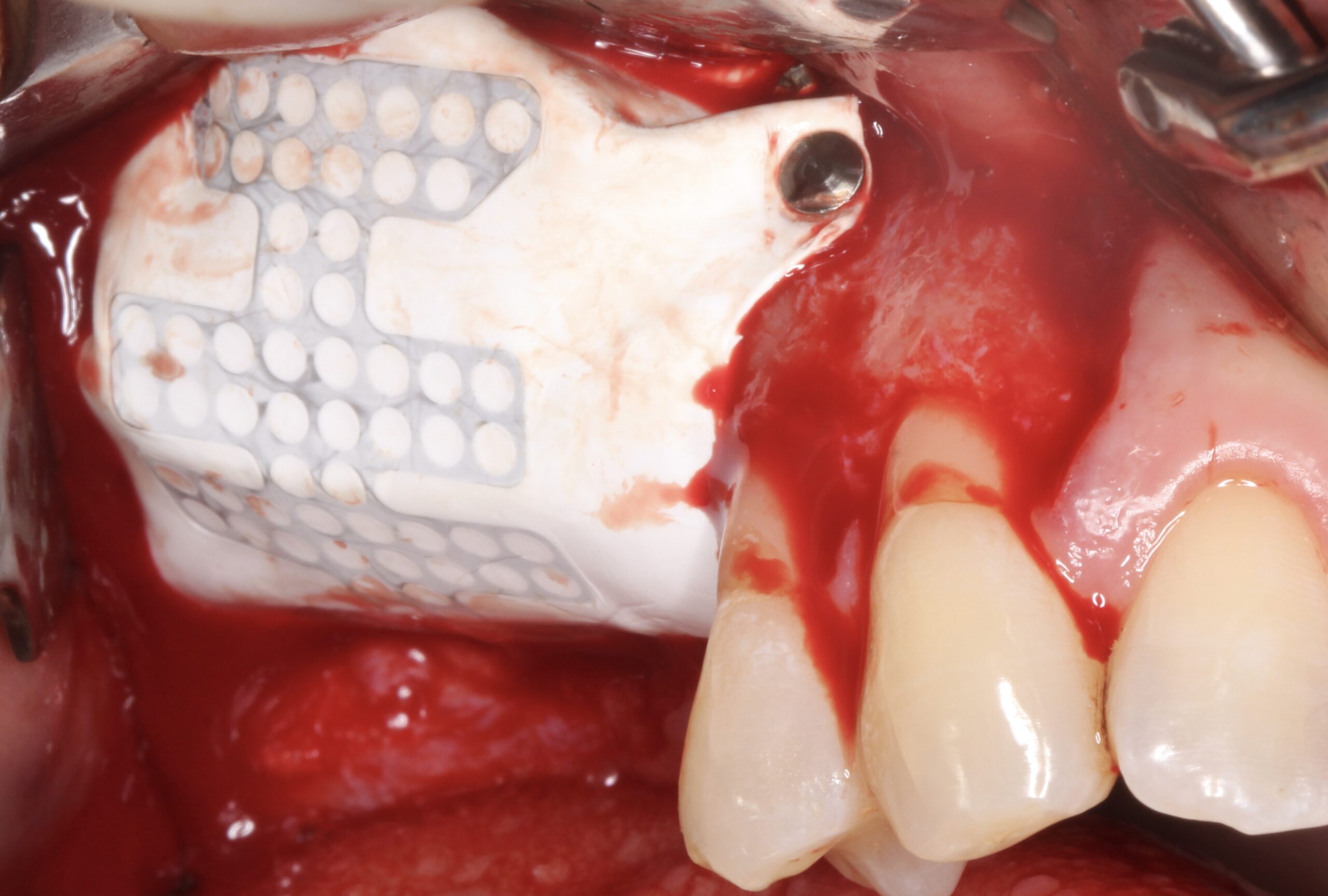
Figure 9.
The membrane was fixed with tacks at buccal aspect covering the ridge trying to gain the maximum possible from the distal bone peak to the maxillary tuberosity.
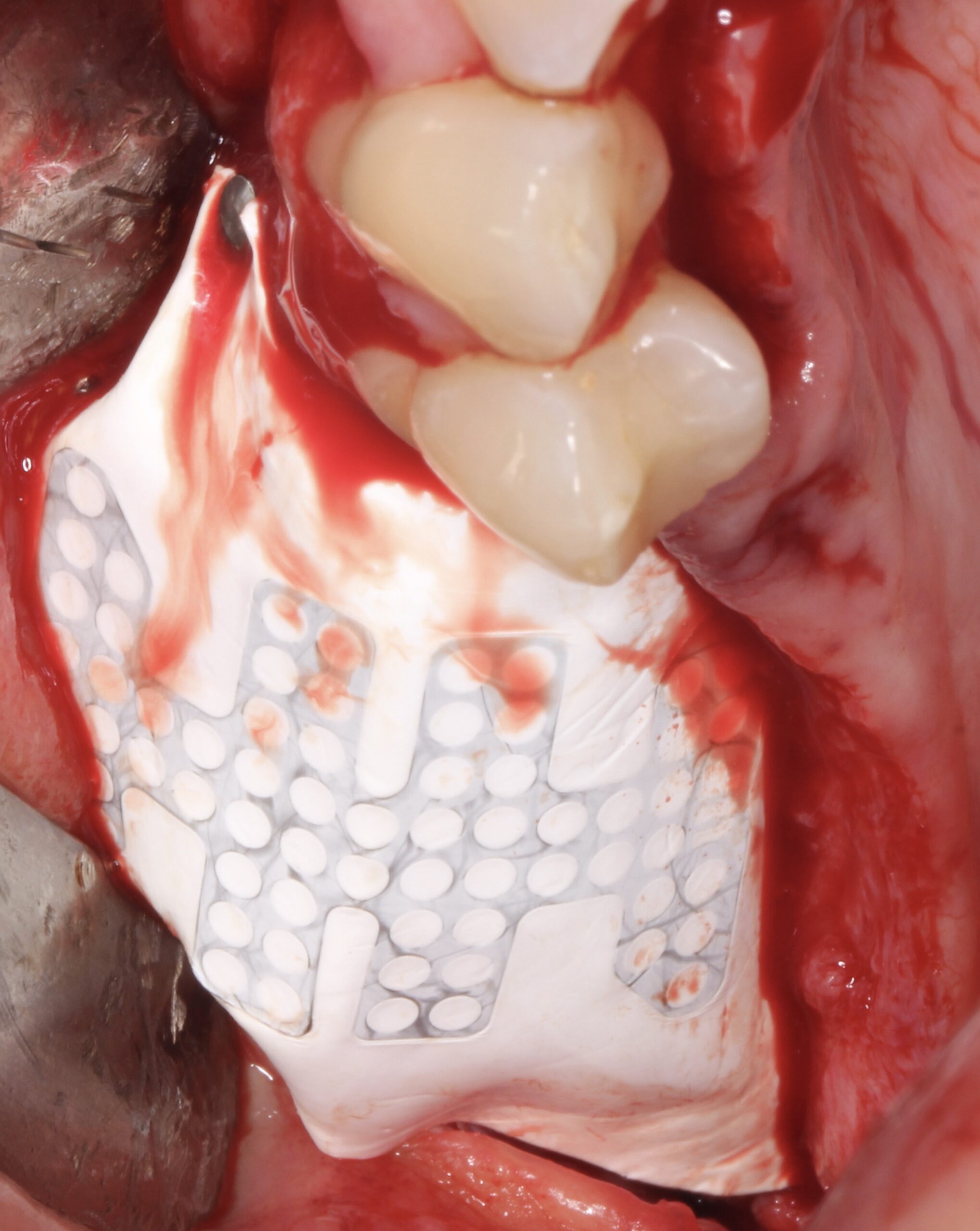
Figure 10.
The membrane was fixed with tacks at buccal aspect covering the ridge trying to gain the maximum possible from the distal bone peak to the maxillary tuberosity.
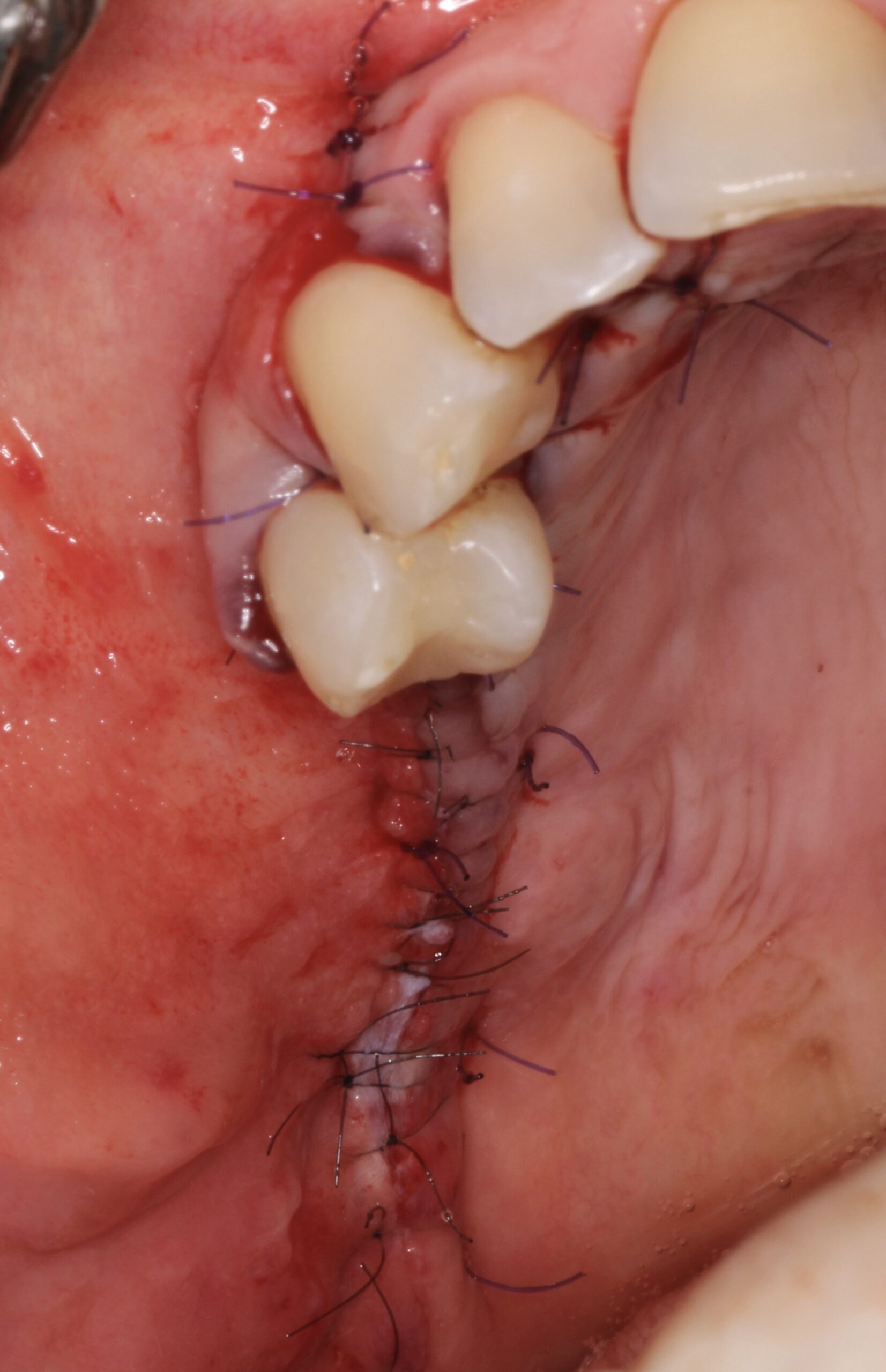
Figure 11.
After realising incisions on the periosteum, primary tension-free closure was achieved by mattress sutures and then interrupted sutures.

Figure 12.
1 year after the GBR surgery, reentry was carried out.
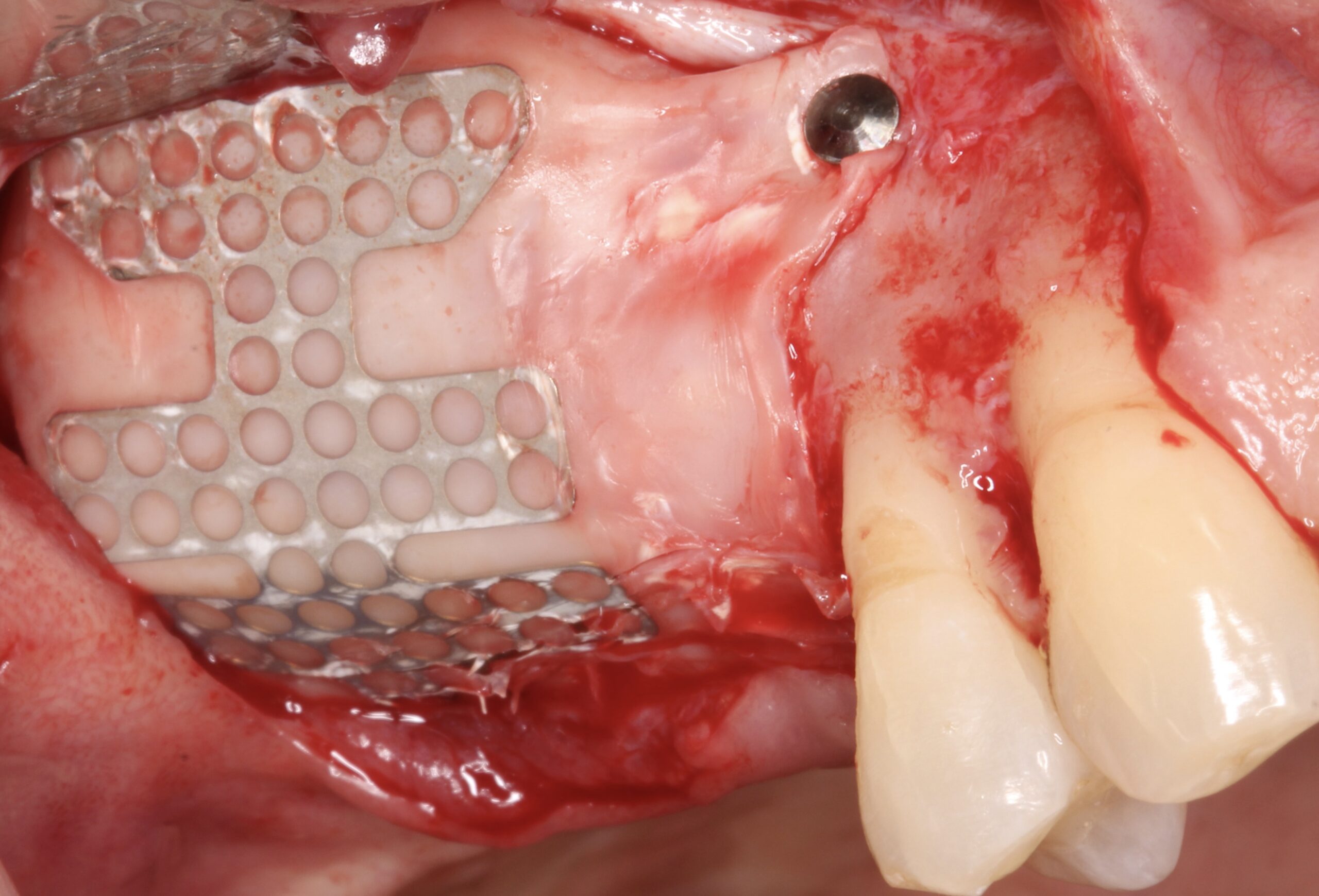
Figure 13.
After raising the flap, the membrane was firm at position.
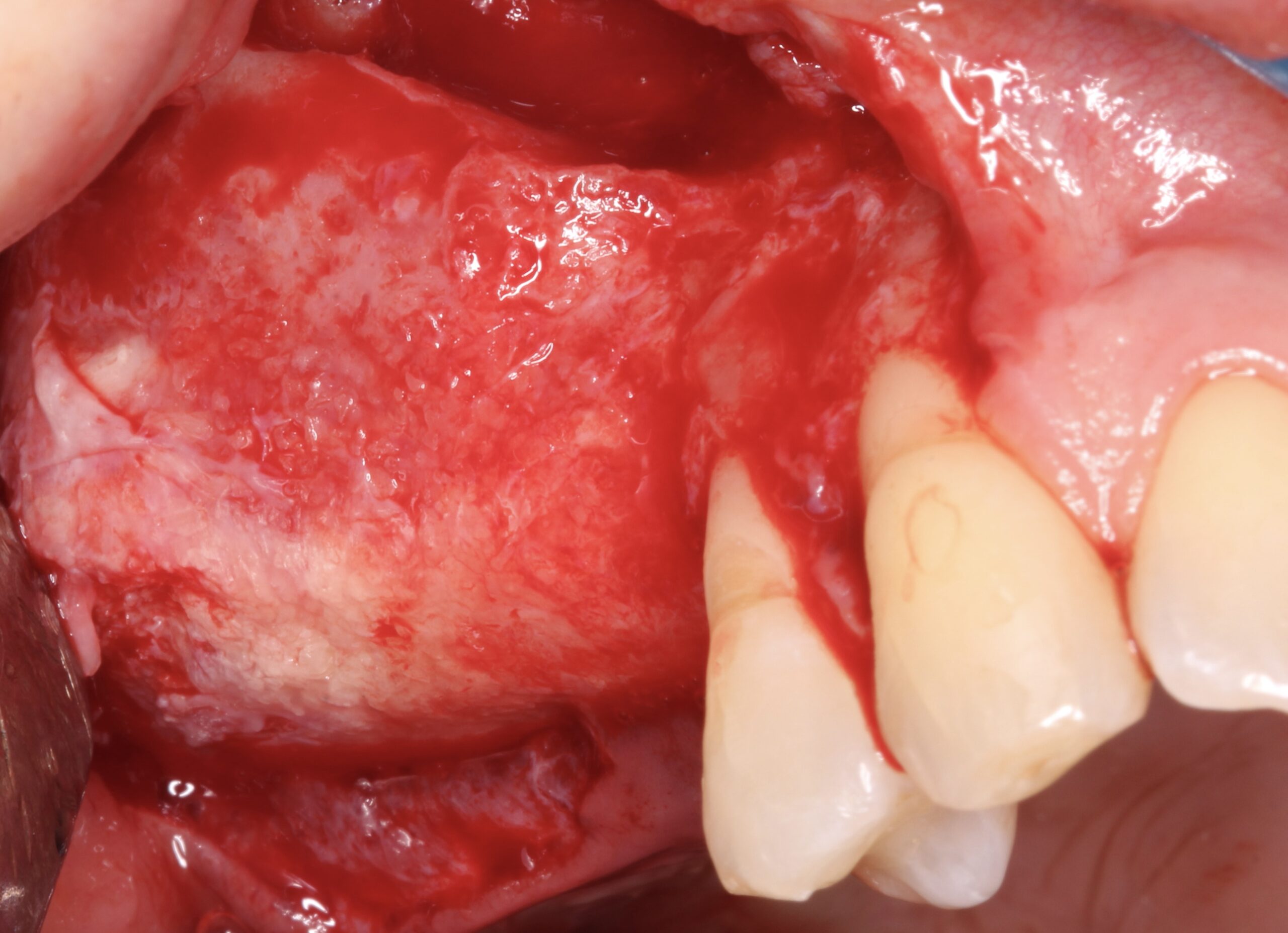
Figure 14.
After removing the membrane it was evident that complete 3D bone regeneration was achieved.
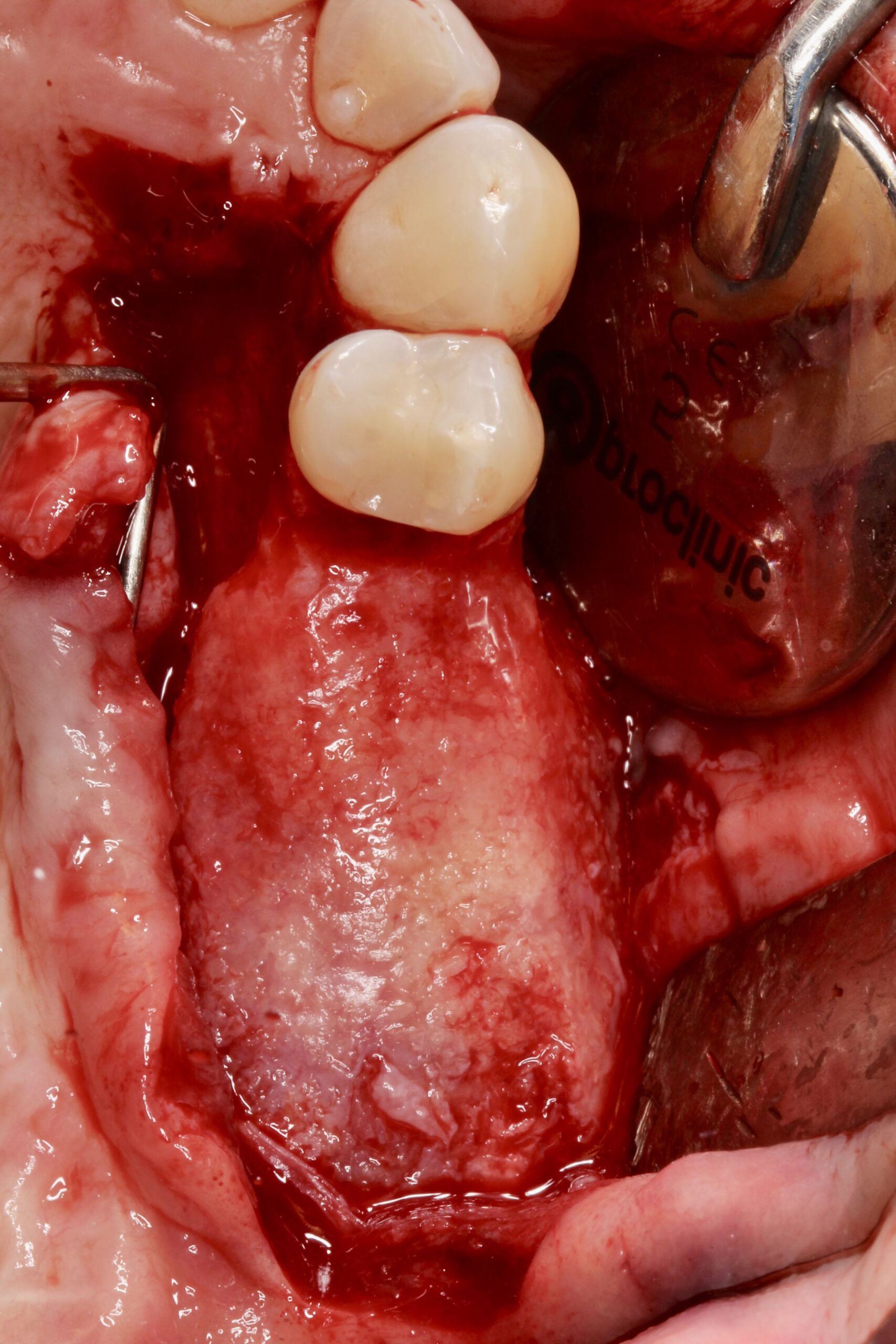
Figure 15.
After removing the membrane it was evident that complete 3D bone regeneration was achieved.
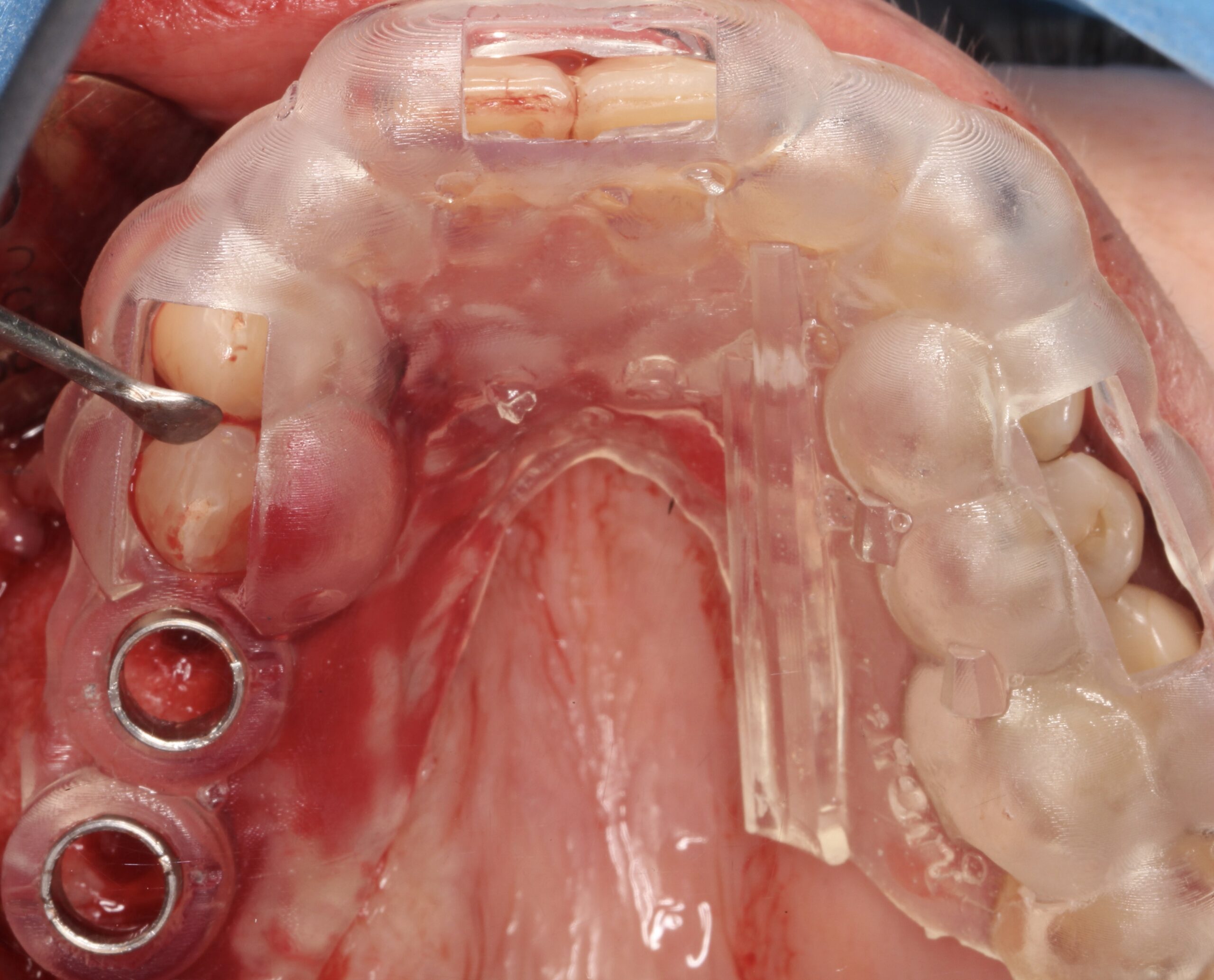
Figure 16.
Using a digital surgical guide.
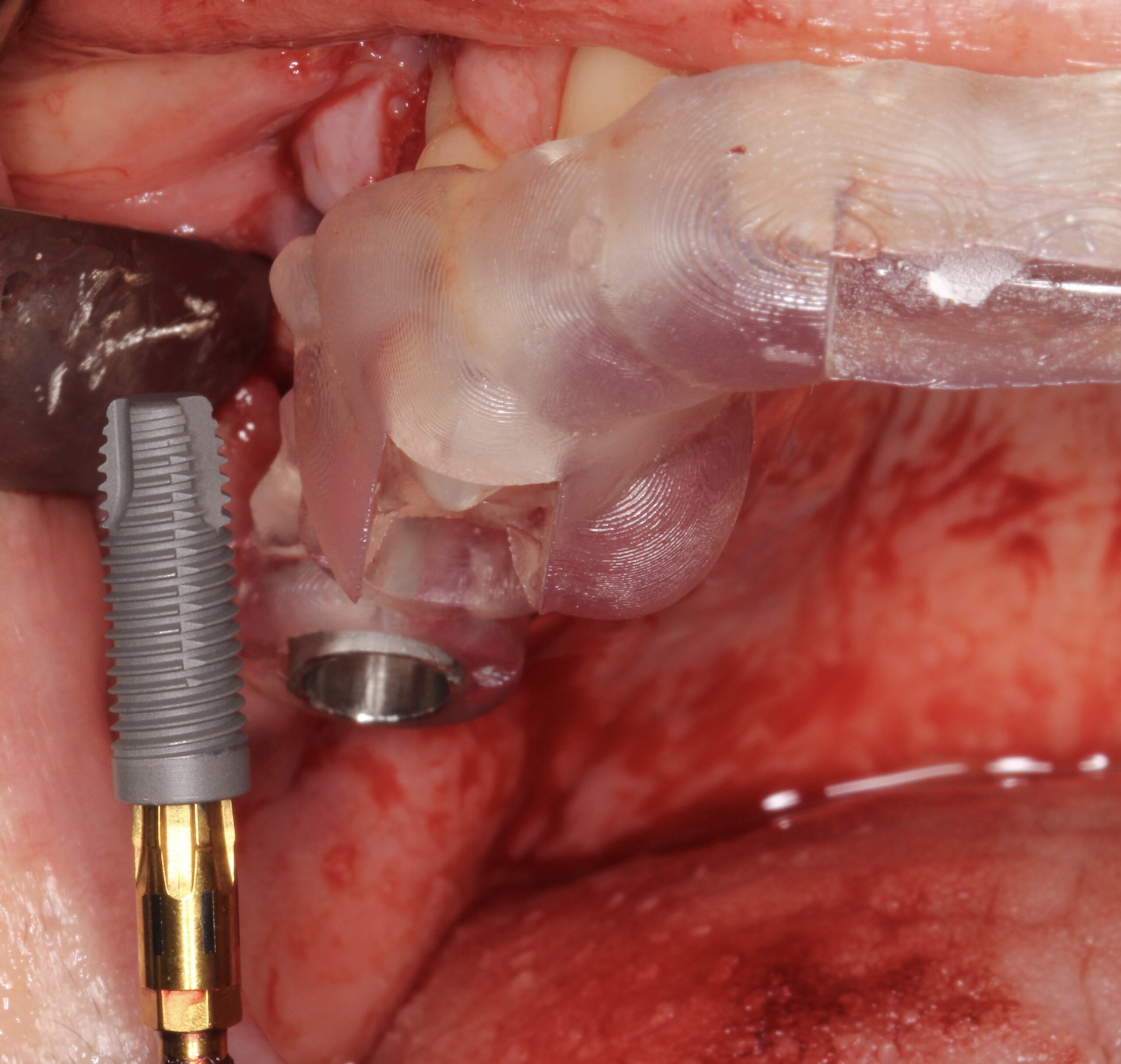
Figure 17.
Two 4.5 mm x 13 mm Neoss ProActive® implants were placed.
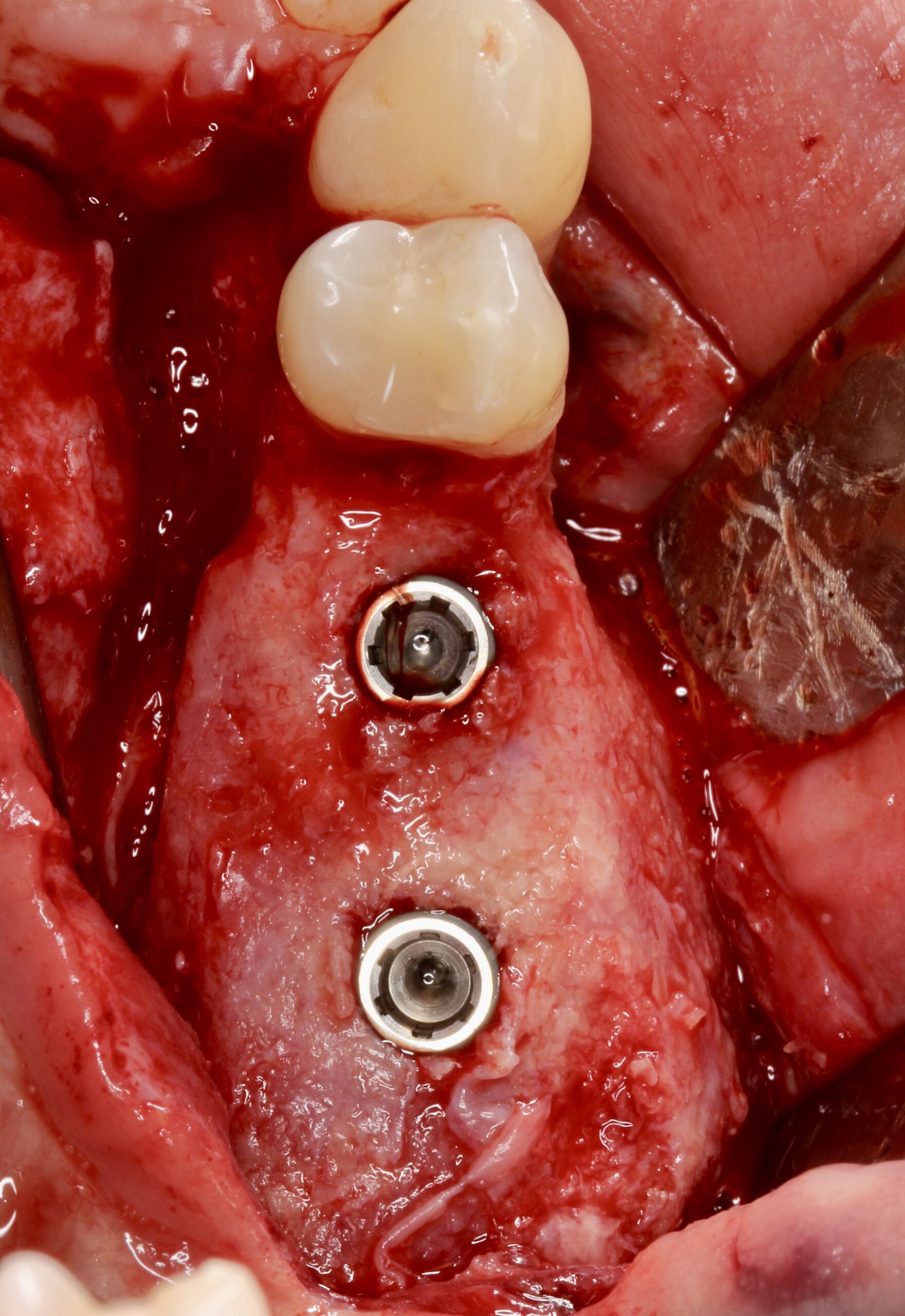
Figure 18.
Placed at 16 and 17 positions.
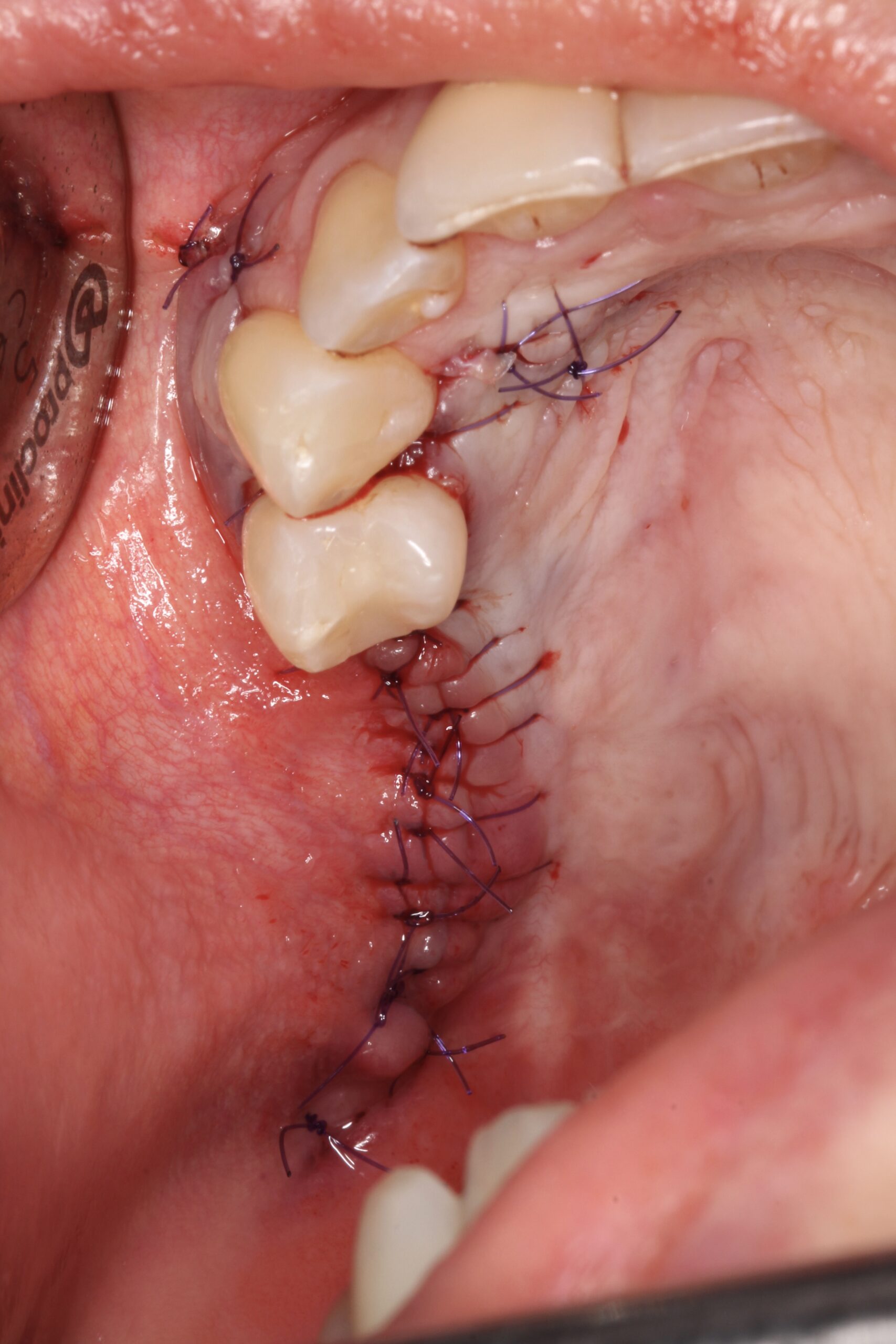
Figure 19.
The implants were submerged during healing osseointegration period.

Figure 20.
2 months later it was evident that there was no keratinised mucosa at buccal aspect and in fact even on the supracrestal area lack of keratinised mucosa was observed.
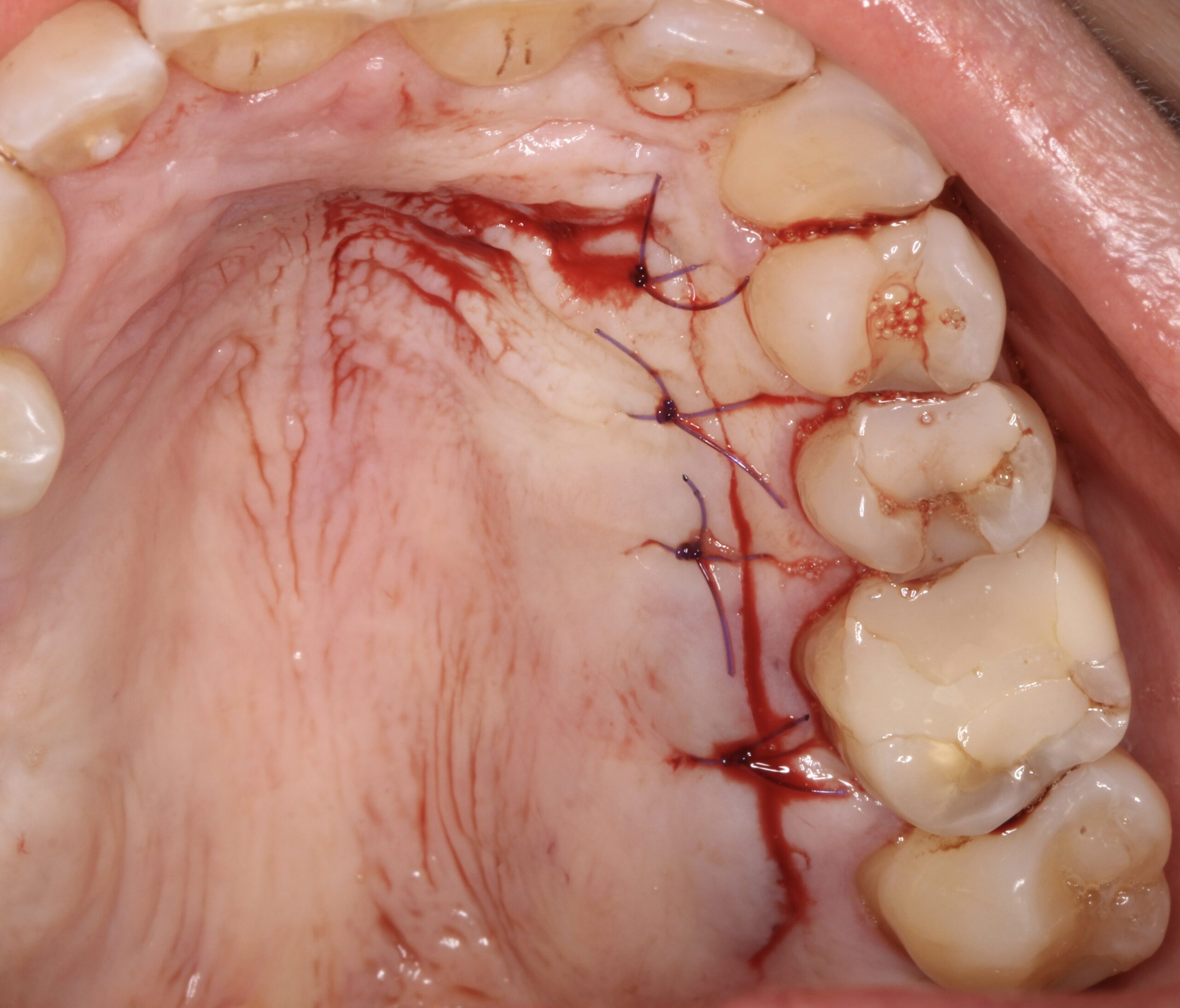
Figure 21.
A connective tissue graft was harvested using a trap-door from the contralateral side of the palate.
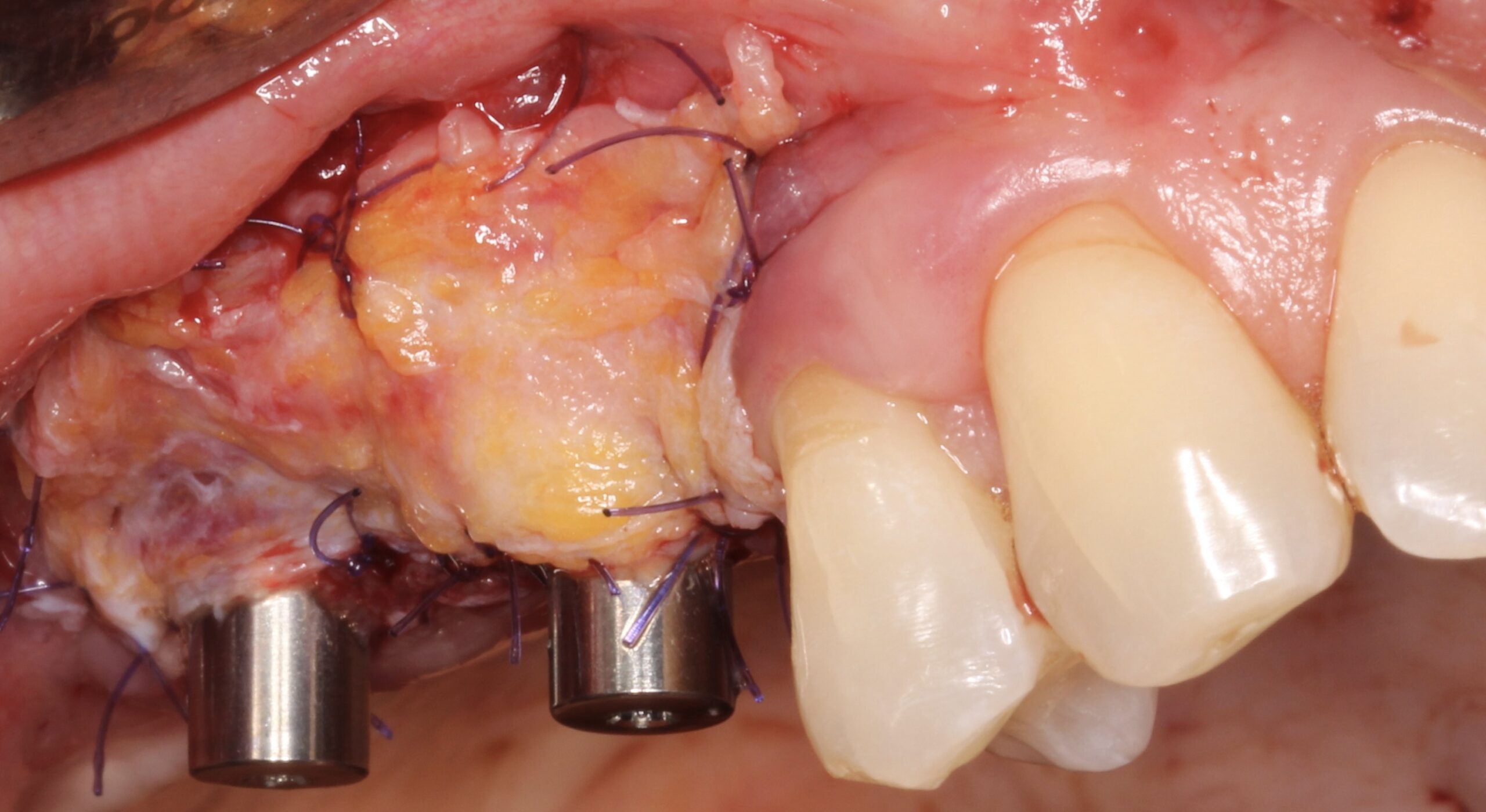
Figure 22.
2nd surgical phase was carried out and at the same time after raising a split-thickness flap the connective tissue graft was placed.
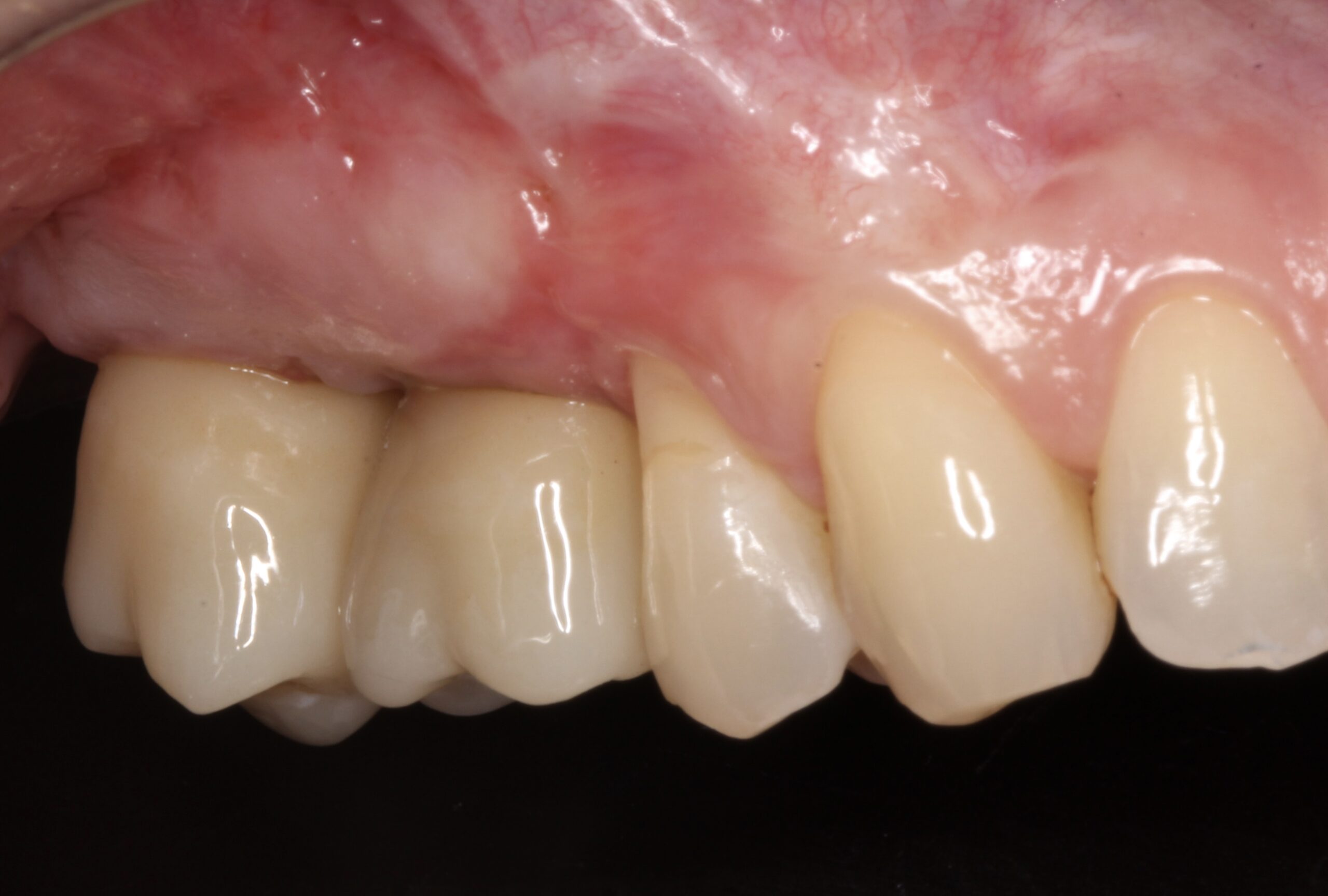
Figure 23.
1 year later clinical status of the implants and crowns was healthy.
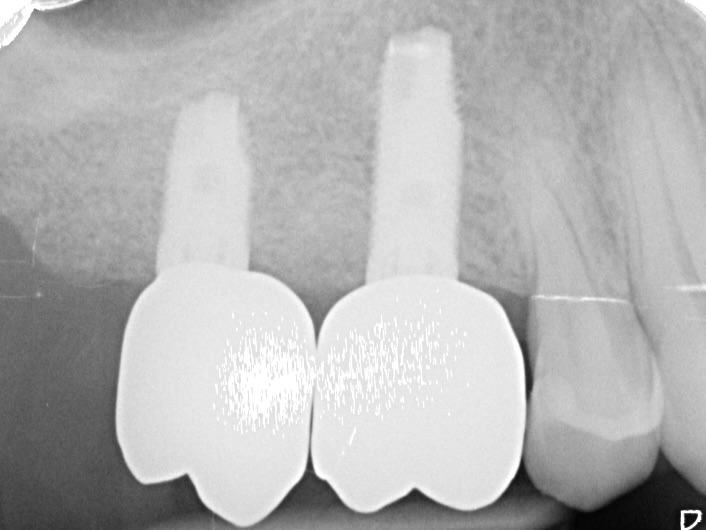
Figure 24.
1 year later radiographic status of the implants and crowns was healthy.
"Neoss ProActive® implant and NeoGen® non-resorbable, Ti-reinforced membrane is an excellent choice for the treatment of atrophic alveolar bone ridge on the aesthetic zone. The solution of bone dehiscences after implant placement by simultaneous GBR by using this protocol is fully predictable.
Dr. David González Spain 
Downloads
