Step by step

Figure 1.
The patient presented with a failing upper left first pre-molar. The CBCT shows the initial situation (Figure 1).
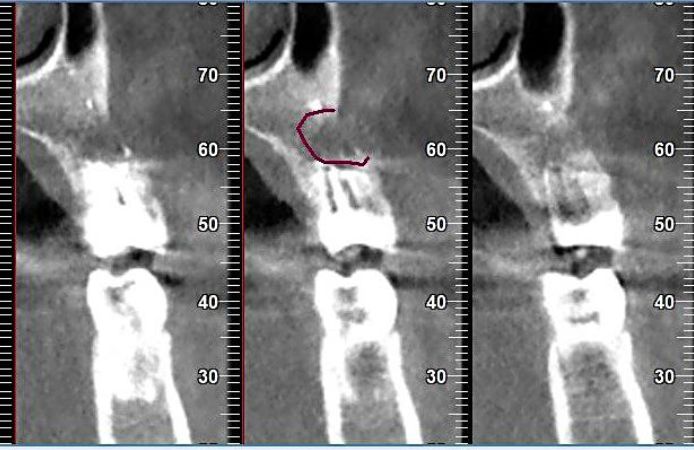
Figure 2.
Note what seems to be a big buccal fenestration in the area of the resected root (Figure 2).

Figure 3.
The broken tooth was extracted (Figure 3–4).

Figure 4.
The broken tooth was extracted (Figure 3–4).
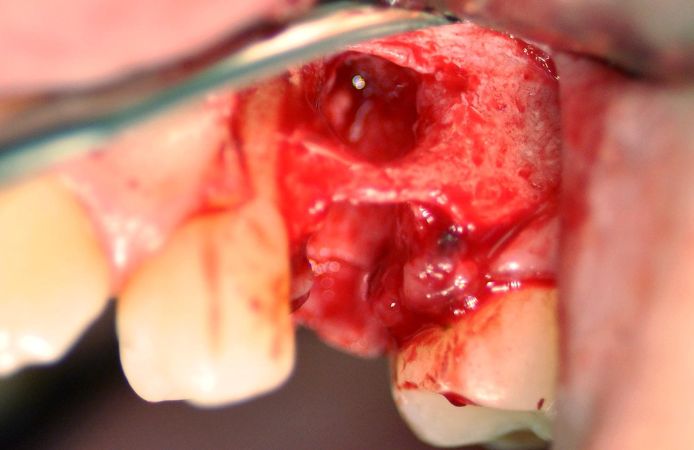
Figure 5.
An access flap was lifted, revealing the buccal fenestration (Figure 5).
Figure 6.
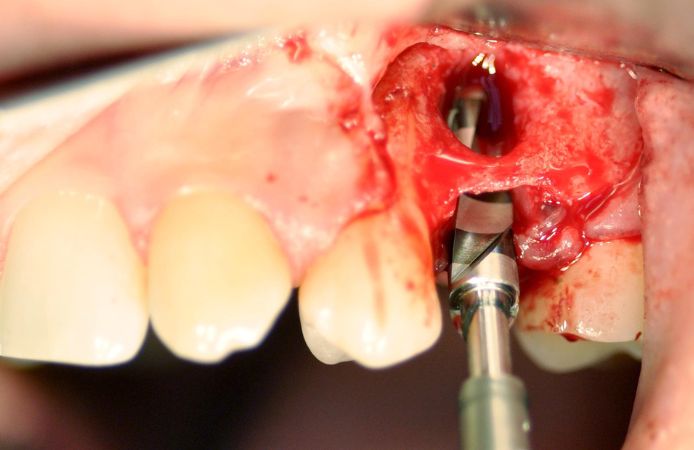
The osteotomy was prepared according to the Neoss ProActive® Edge drill protocol (Figure 6).

Figure 7.
Placement of one ∅5.0 × 13 mm Neoss ProActive® Edge implant (Figure 7).
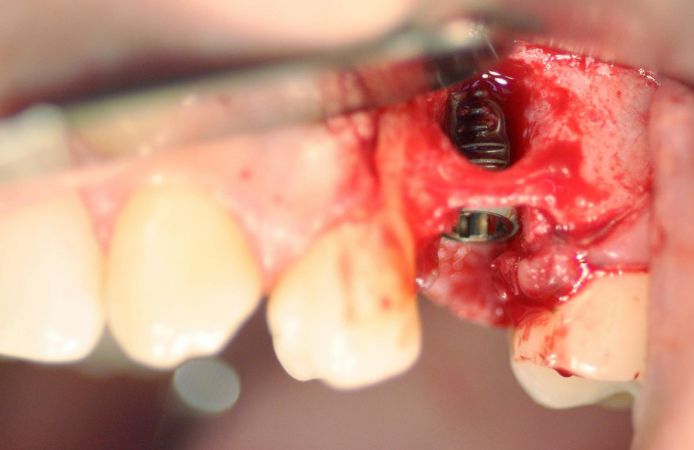
Figure 8.
The implant was placed in very limited bone quantity of medium bone density (Figure 8). Good primary stability was reached despite the limited bone situation. The insertion torque was 20 Ncm and ISQ was 70/77.

Figure 9.
THE Graft (Purgo) cancellous bone granules (Figure 9) were used to correct the buccal fenestration (Figure 10).

Figure 10.
THE Graft (Purgo) cancellous bone granules (Figure 9) were used to correct the buccal fenestration (Figure 10).

Figure 11.
The bone graft was covered with a resorbable collagen membrane (Figure 11).

Figure 12.
The mucosal flap was sutured around the PEEK healing abutment, allowing for one-stage healing (Figure 12).

Figure 13.
Radiograph showing the implant at time of insertion (Figure 13).

Figure 14.
A Neoss ScanPeg was attached to the healing abutment (Figure 14), and the site was digitally scanned using an intraoral scanner (Figure 15).
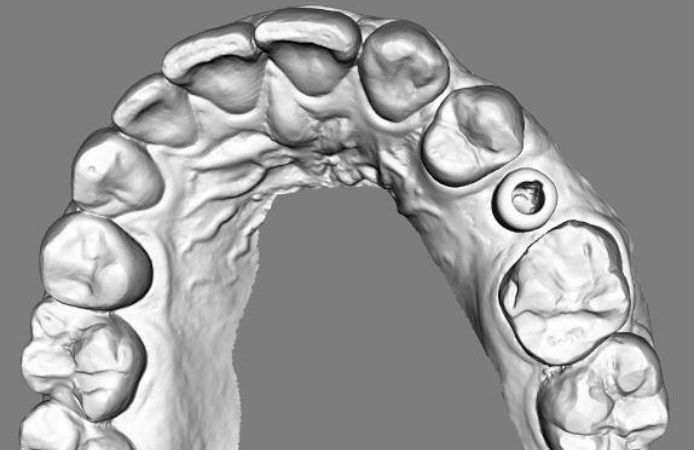
Figure 15.
A Neoss ScanPeg was attached to the healing abutment (Figure 14), and the site was digitally scanned using an intraoral scanner (Figure 15).
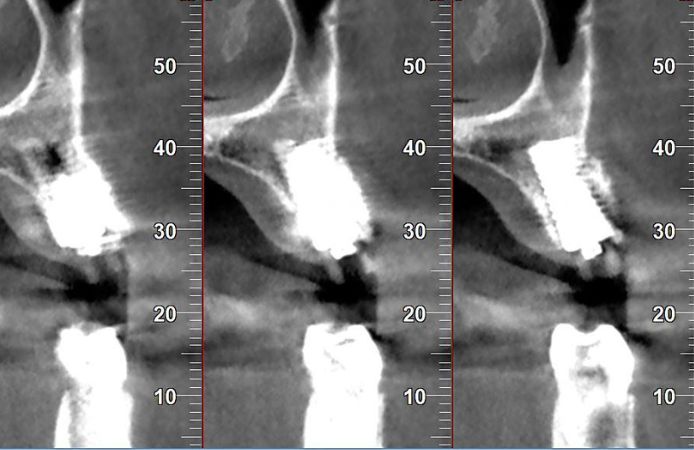
Figure 16.
The CBCT after 3.5 months healing (Figure 16) shows good integration of the Edge implant and bone regeneration in the initial defect. The ISQ had increased to 72/79 further indicating good integration.

Figure 17.
Using a completely digital workflow, an individualized zirconia abutment was fabricated on a Neoss TiBase (Figure 17) and a zirconia crown was fitted on the abutment (Figure 18).

Figure 18.
Using a completely digital workflow, an individualized zirconia abutment was fabricated on a Neoss TiBase (Figure 17) and a zirconia crown was fitted on the abutment (Figure 18).


Downloads
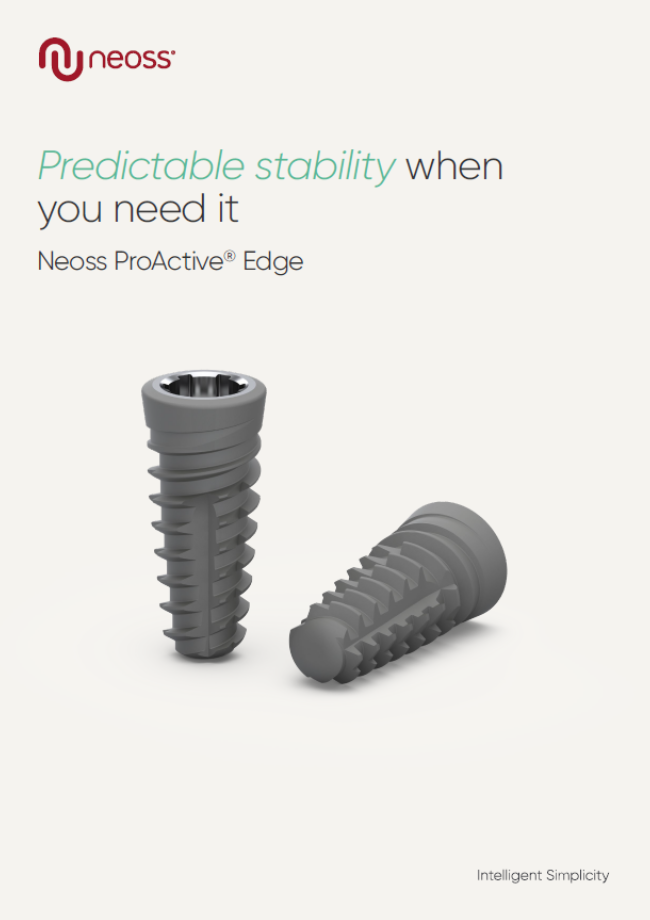
Neoss ProActive Edge
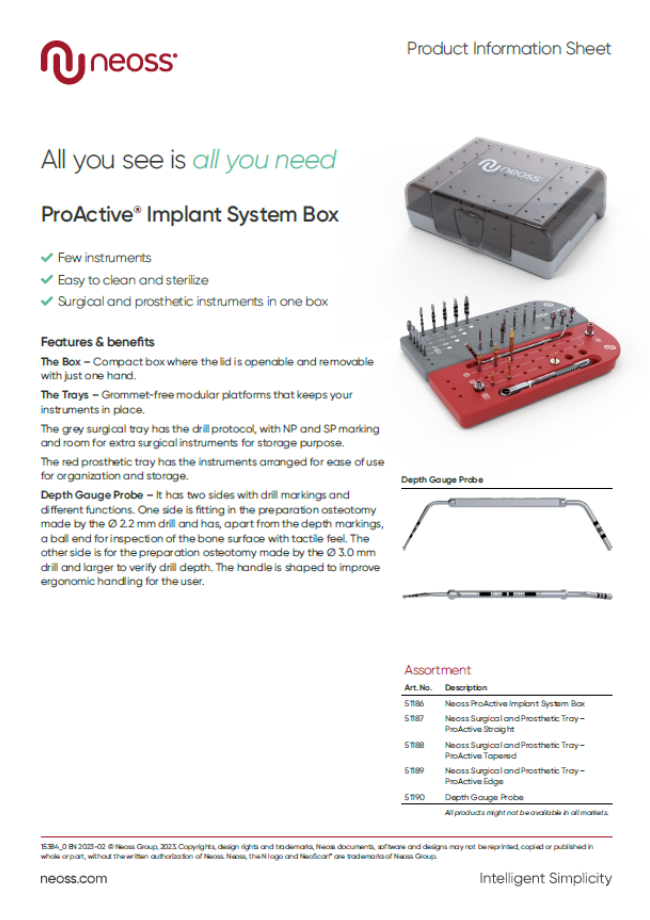
ProActive System Implant Box product sheet
